

Impact of Guidance Provided by a Multispectral Digital Skin Lesion Analysis Device Following Dermoscopy on Decisions to Biopsy Atypical Melanocytic Lesions
- PMID: 26430487
- PMCID: PMC4587891
Impact of Guidance Provided by a Multispectral Digital Skin Lesion Analysis Device Following Dermoscopy on Decisions to Biopsy Atypical Melanocytic Lesions
Abstract
Objective: To determine how a multispectral digital skin lesion analysis (MSDSLA) device data affects the biopsy performance of dermatologists and non-dermatologist practitioners following clinical and dermoscopic pigmented lesion evaluation.
Design: MSDSLA employs near infrared light to image and analyze pigmented skin lesions. MSDSLA generates a "classifier score" based on morphological disorganization. Using a logistical regression model, 1) a probability of being melanoma and, 2) a probability of being melanoma, atypical melanocytic hyperplasia, or a high grade dysplastic nevus is computed. PARTICIPANTS were shown clinical images of 12 lesions (2 melanomas in situ, 3 invasive melanomas, and 7 low grade DNs). They were asked first if they would biopsy the lesion based on clinical images, again after observing dermoscopy images, and once more when presented with MSDSLA probability information.
Setting: National dermoscopy conference.
Participants: Sixty-four healthcare providers; 30 dermatologists and 34 non-dermatologist practitioners.
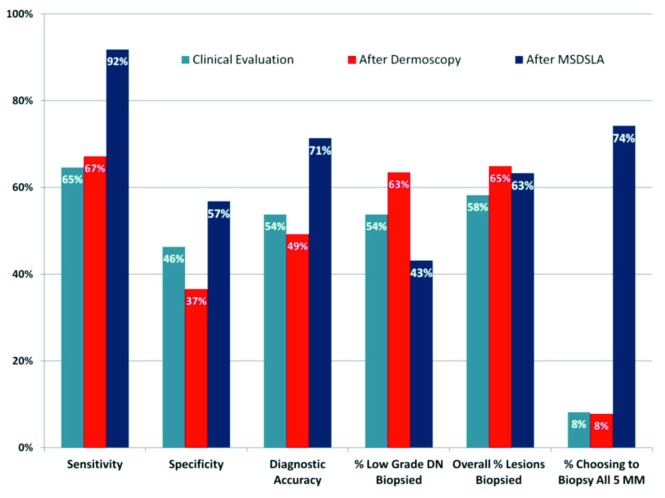
Measurements: Sensitivity, specificity, diagnostic accuracy, biopsy rates Results: For the 30 dermatologists, sensitivity was 65 percent after clinical evaluation (C) and 65% post-dermoscopy (D) but improved to 91% after MSDSLA. For the 34 non-dermatologist practitioners, sensitivity improved from 66 percent (C) to 70 percent (D) to 95 percent after MSDSLA. With MSDSLA information, dermatologist specificity increased from 40 percent (D) to 58 percent while non-dermatologist practitioners specificity increased from 34 percent (D) to 55 percent. Diagnostic accuracy of malignant and benign lesions decreased for both groups 55 percent (C) to 51 percent (D) for dermatologists and 54 percent (C) to 49 percent (D) for non-dermatologist practitioners. However, diagnostic accuracy increased to 72 percent for dermatologists and 72 percent for non-dermatologist practitioners with MSDSLA data. Non-melanoma biopsy percentages by dermatologists increased from 53 percent (C) to 60 percent (D), but decreased to 42 percent when provided with MSDSLA data. Similarly, non-dermatologist practitioners' biopsy percentages of nonmelanomas increased from 55 percent (C) to 66 percent (D) and decreased to 45 percent with MSDSLA.
Conclusion: Decisions to biopsy atypical melanocytic lesions were more sensitive and specific when MSDSLA information was provided for both dermatologists and nondermatologist practitioners. Both groups were also less likely to biopsy nonmelanomas after MSDSLA evaluation. The authors' results suggest providing practitioners with MSDSLA data leads to improved biopsy accuracy decreasing the number of nonessential biopsies for nonmelanocytic lesions even after dermoscopic evaluation.
Figures
References
-
- Gloster HM, Jr, Brodland DG. The epidemiology of skin cancer. Dermatol Surg. 1996;22:217–226. - PubMed
-
- Wang SQ, Kopf AW, Koenig K, et al. Detection of melanomas in patients followed up with total cutaneous examinations, total cutaneous photography, and dermoscopy. J Am Acad Dermatol. 2004;50:15–20. - PubMed
-
- Ruocco E, Argenziano G, Pellacani G, et al. Noninvasive imaging of skin tumors. Dermatol Surg. 2004;30p2:301–310. - PubMed
-
- Gutkowicz-Krusin D, Elbaum M, Jacobs A, et al. Precision of automatic measurements of pigmented skin lesion para¬meters with a MelaFind multispectral digital dermoscope. Melanoma Res. 2000;10:563–570. - PubMed
-
- Monheit G, Cognetta AB, Ferris L, et al. The performance of MelaFind: a prospective multicenter study. Arch Dermatol. 2011;147:188–194. - PubMed
LinkOut - more resources
Full Text Sources