

Lateral Brow Lift: A Multi-Point Suture Fixation Technique
- PMID: 26430629
- PMCID: PMC4579169
- DOI: 10.5999/aps.2015.42.5.580
Lateral Brow Lift: A Multi-Point Suture Fixation Technique
Abstract
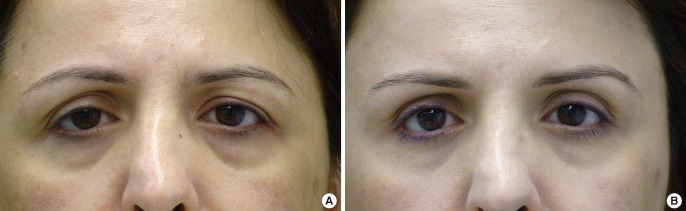
Background: Descent of the lateral aspect of the brow is one of the earliest signs of aging. The purpose of this study was to describe an open surgical technique for lateral brow lifts, with the goal of achieving reliable, predictable, and long-lasting results.
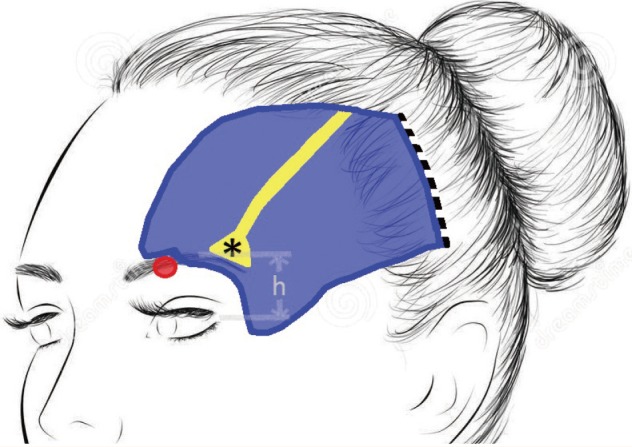
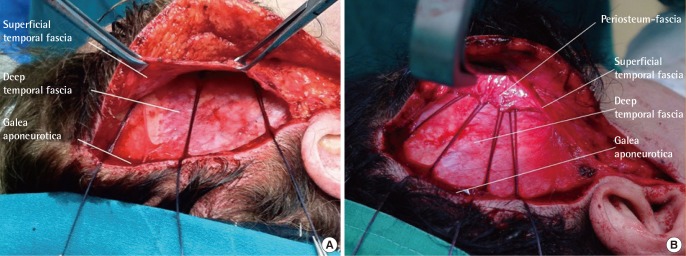
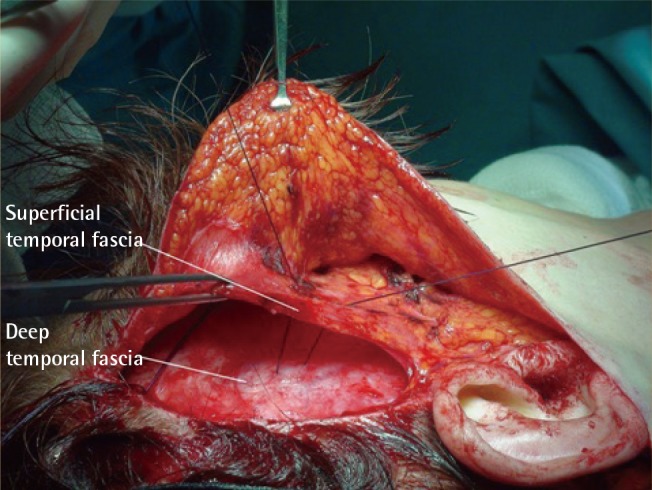
Methods: An incision was made behind and parallel to the temporal hairline, and then extended deeper through the temporoparietal fascia to the level of the deep temporal fascia. Dissection was continued anteriorly on the surface of the deep temporal fascia and subperiosteally beyond the temporal crest, to the level of the superolateral orbital rim. Fixation of the lateral brow and tightening of the orbicularis oculi muscle was achieved with the placement of sutures that secured the tissue directly to the galea aponeurotica on the lateral aspect of the incision. An additional fixation was made between the temporoparietal fascia and the deep temporal fascia, as well as between the temporoparietal fascia and the galea aponeurotica. The excess skin in the temporal area was excised and the incision was closed.
Results: A total of 519 patients were included in the study. Satisfactory lateral brow elevation was obtained in most of the patients (94.41%). The following complications were observed: total relapse (n=8), partial relapse (n=21), neurapraxia of the frontal branch of the facial nerve (n=5), and limited alopecia in the temporal incision (n=9).
Conclusions: We consider this approach to be a safe and effective procedure, with long-lasting results.
Keywords: Eyebrow; Rejuvenation; Surgery, plastic; Sutures.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures





References
-
- Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg. 1996;97:1321–1333. - PubMed
-
- Chiu ES, Baker DC. Endoscopic brow lift: a retrospective review of 628 consecutive cases over 5 years. Plast Reconstr Surg. 2003;112:628–633. - PubMed
-
- Gleason MC. Brow lifting through a temporal scalp approach. Plast Reconstr Surg. 1973;52:141–144. - PubMed
-
- Paul MD. The evolution of the brow lift in aesthetic plastic surgery. Plast Reconstr Surg. 2001;108:1409–1424. - PubMed
-
- Gasperoni C, Salgarello M, Gargani G. Subperiosteal lateral browlift and its relationship to upper blepharoplasty. Aesthetic Plast Surg. 1993;17:243–246. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources