

Biofilm formation is a risk factor for mortality in patients with Candida albicans bloodstream infection-Scotland, 2012-2013
- PMID: 26432192
- PMCID: PMC4721535
- DOI: 10.1016/j.cmi.2015.09.018
Biofilm formation is a risk factor for mortality in patients with Candida albicans bloodstream infection-Scotland, 2012-2013
Abstract
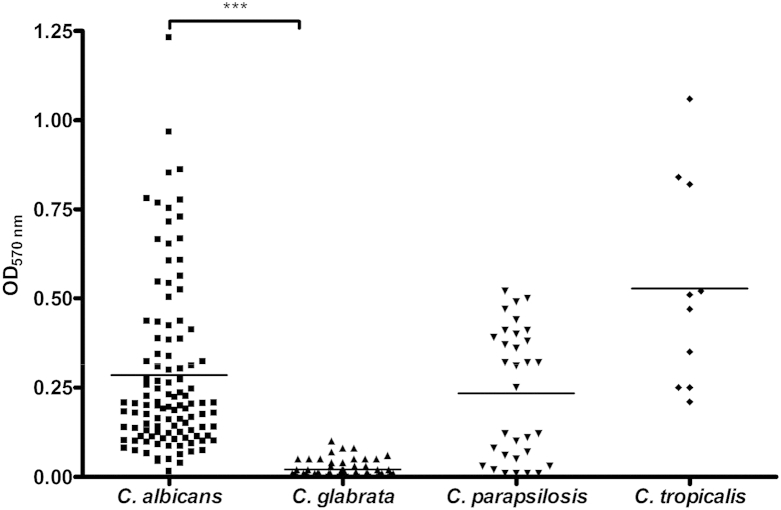
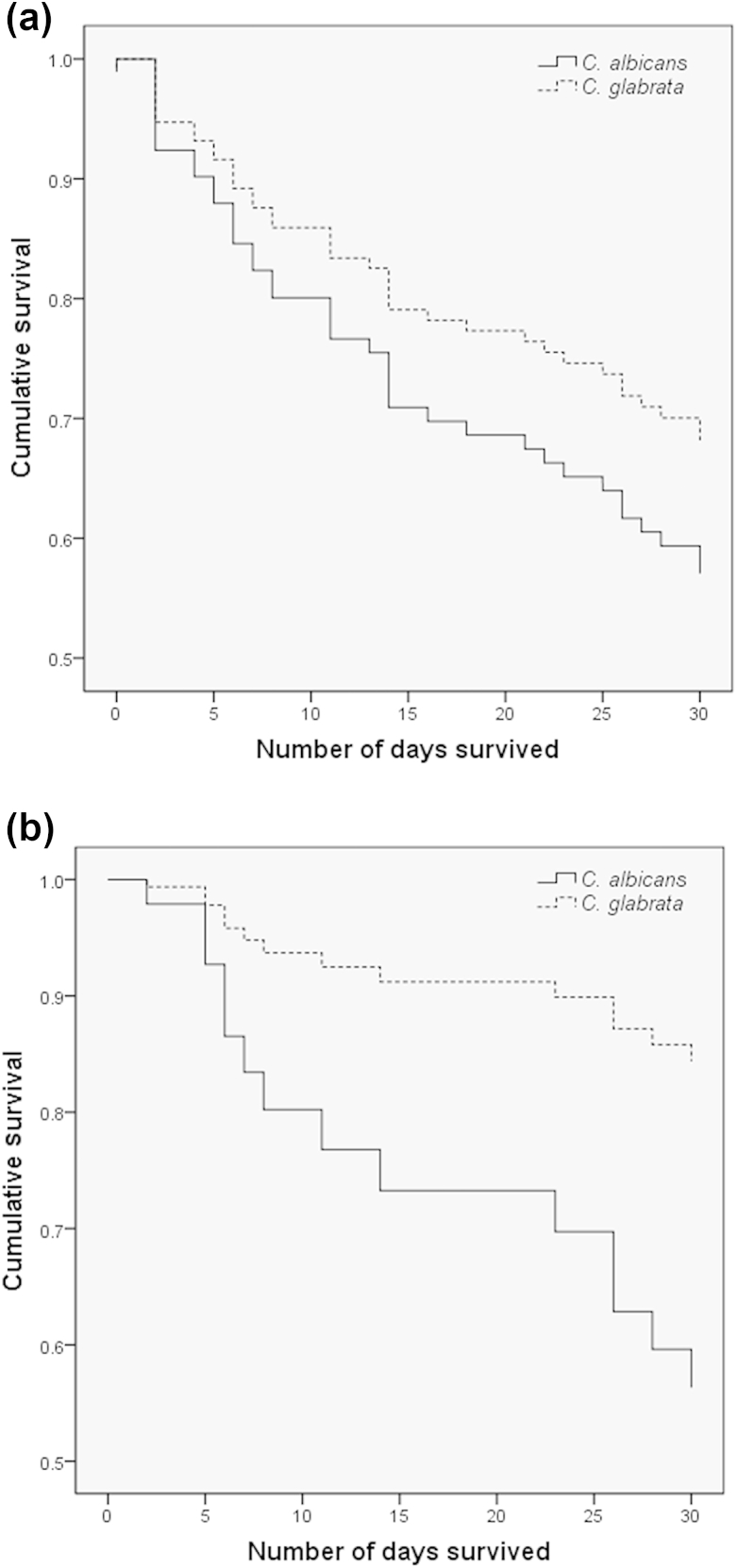
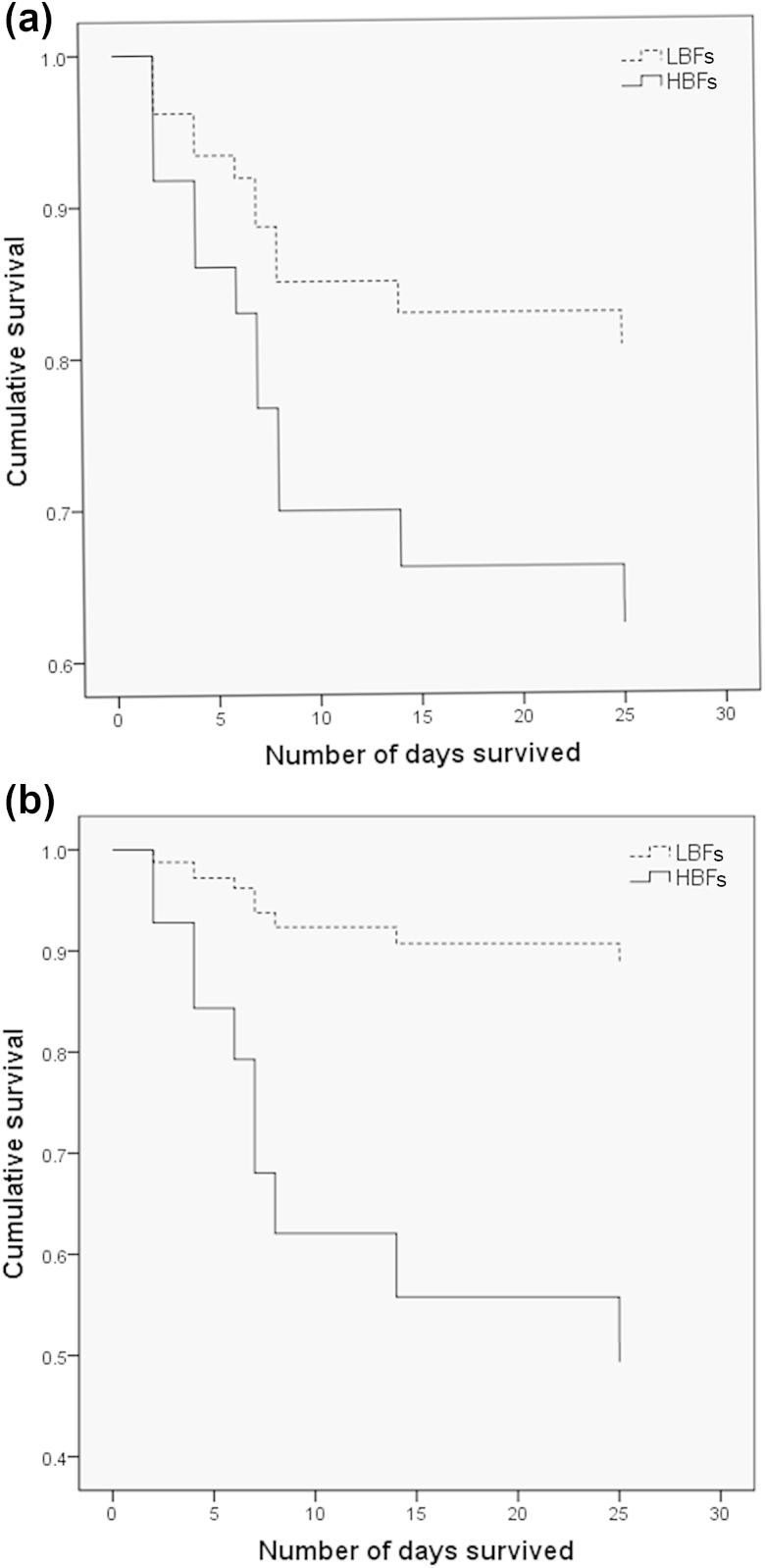
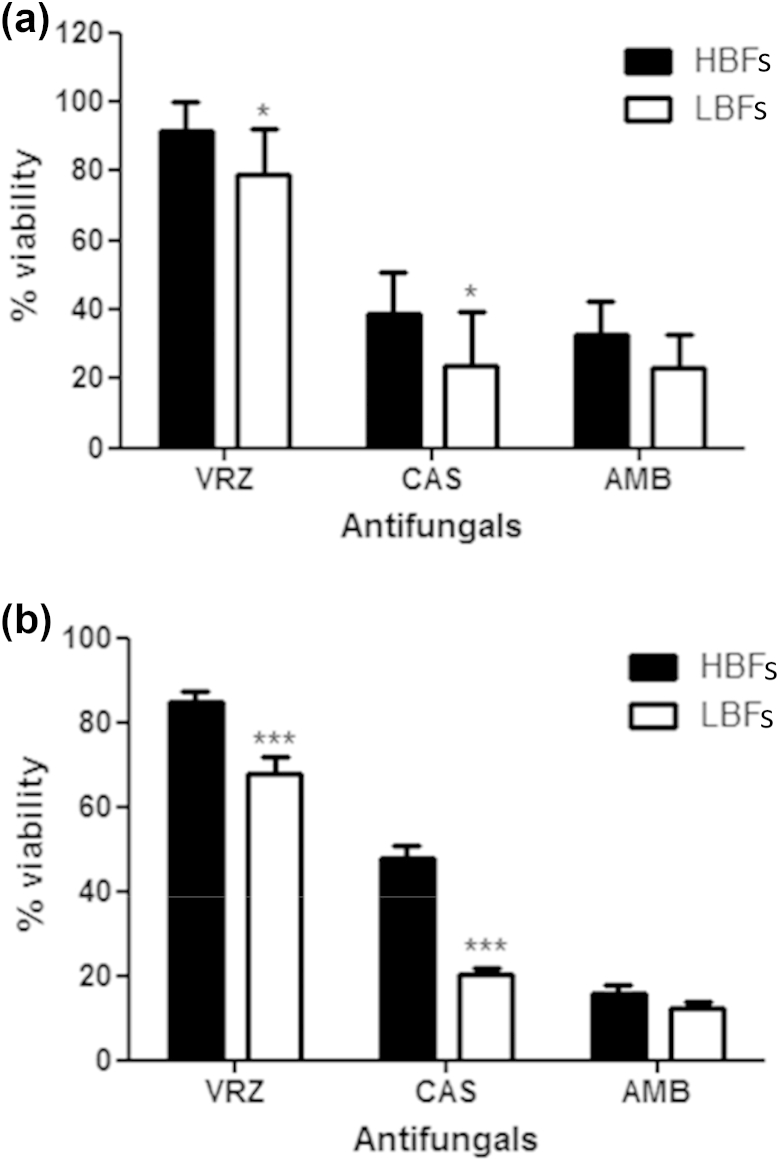
Bloodstream infections caused by Candida species remain a significant cause of morbidity and mortality in hospitalized patients. Biofilm formation by Candida species is an important virulence factor for disease pathogenesis. A prospective analysis of patients with Candida bloodstream infection (n = 217) in Scotland (2012-2013) was performed to assess the risk factors associated with patient mortality, in particular the impact of biofilm formation. Candida bloodstream isolates (n = 280) and clinical records for 157 patients were collected through 11 different health boards across Scotland. Biofilm formation by clinical isolates was assessed in vitro with standard biomass assays. The role of biofilm phenotype on treatment efficacy was also evaluated in vitro by treating preformed biofilms with fixed concentrations of different classes of antifungal. Available mortality data for 134 patients showed that the 30-day candidaemia case mortality rate was 41%, with predisposing factors including patient age and catheter removal. Multivariate Cox regression survival analysis for 42 patients showed a significantly higher mortality rate for Candida albicans infection than for Candida glabrata infection. Biofilm-forming ability was significantly associated with C. albicans mortality (34 patients). Finally, in vitro antifungal sensitivity testing showed that low biofilm formers and high biofilm formers were differentially affected by azoles and echinocandins, but not by polyenes. This study provides further evidence that the biofilm phenotype represents a significant clinical entity, and that isolates with this phenotype differentially respond to antifungal therapy in vitro. Collectively, these findings show that greater clinical understanding is required with respect to Candida biofilm infections, and the implications of isolate heterogeneity.
Keywords: Antifungal; Candida albicans; Candida glabrata; biofilm; candidaemia; catheters; drug resistance.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Mensa J., Pitart C., Marco F. Treatment of critically ill patients with candidemia. Int J Antimicrob Agents. 2008;32(Suppl. 2):S93–S97. - PubMed
-
- Wisplinghoff H., Bischoff T., Tallent S.M., Seifert H., Wenzel R.P., Edmond M.B. Nosocomial bloodstream infections in US hospitals: Analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39:309–317. - PubMed
-
- Lynch A.S., Robertson G.T. Bacterial and fungal biofilm infections. Annu Rev Med. 2008;59:415–428. - PubMed
-
- Sardi J.C., Scorzoni L., Bernardi T., Fusco-Almeida A.M., Mendes Giannini M.J. Candida species: Current epidemiology, pathogenicity, biofilm formation, natural antifungal products and new therapeutic options. J Med Microbiol. 2013;62(Pt 1):10–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
