

European Myeloma Network guidelines for the management of multiple myeloma-related complications
- PMID: 26432383
- PMCID: PMC4591757
- DOI: 10.3324/haematol.2014.117176
European Myeloma Network guidelines for the management of multiple myeloma-related complications
Abstract
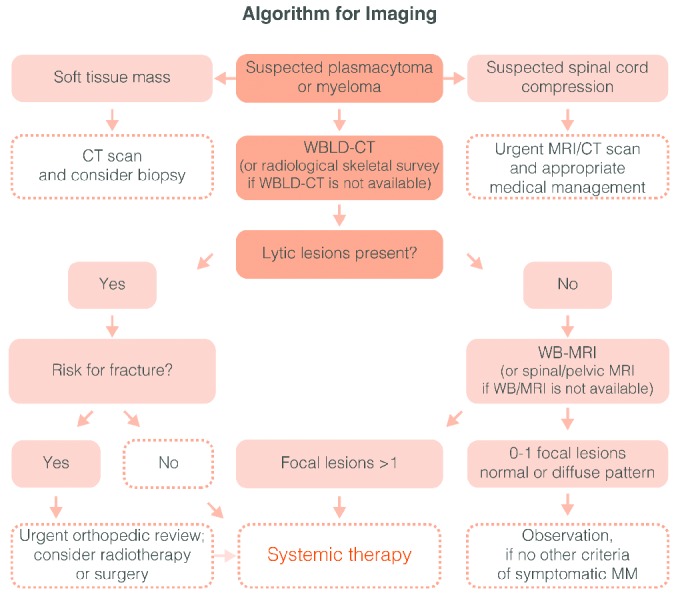
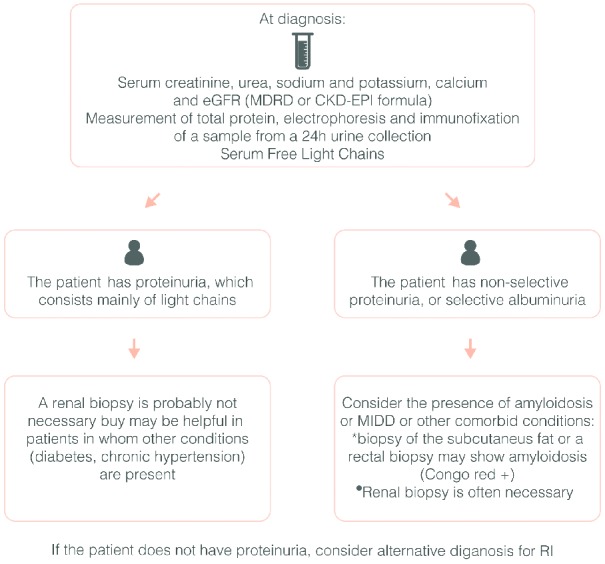
The European Myeloma Network provides recommendations for the management of the most common complications of multiple myeloma. Whole body low-dose computed tomography is more sensitive than conventional radiography in depicting osteolytic disease and thus we recommend it as the novel standard for the detection of lytic lesions in myeloma (grade 1A). Myeloma patients with adequate renal function and bone disease at diagnosis should be treated with zoledronic acid or pamidronate (grade 1A). Symptomatic patients without lytic lesions on conventional radiography can be treated with zoledronic acid (grade 1B), but its advantage is not clear for patients with no bone involvement on computed tomography or magnetic resonance imaging. In asymptomatic myeloma, bisphosphonates are not recommended (grade 1A). Zoledronic acid should be given continuously, but it is not clear if patients who achieve at least a very good partial response benefit from its continuous use (grade 1B). Treatment with erythropoietic-stimulating agents may be initiated in patients with persistent symptomatic anemia (hemoglobin <10g/dL) in whom other causes of anemia have been excluded (grade 1B). Erythropoietic agents should be stopped after 6-8 weeks if no adequate hemoglobin response is achieved. For renal impairment, bortezomib-based regimens are the current standard of care (grade 1A). For the management of treatment-induced peripheral neuropathy, drug modification is needed (grade 1C). Vaccination against influenza is recommended; vaccination against streptococcus pneumonia and hemophilus influenza is appropriate, but efficacy is not guaranteed due to suboptimal immune response (grade 1C). Prophylactic aciclovir (or valacyclovir) is recommended for patients receiving proteasome inhibitors, autologous or allogeneic transplantation (grade 1A).
Copyright© Ferrata Storti Foundation.
Figures

References
-
- Terpos E, Dimopoulos MA. Myeloma bone disease: pathophysiology and management. Ann Oncol. 2005;16(8):1223–1231. - PubMed
-
- Dimopoulos M, Terpos E, Comenzo RL, et al. International myeloma working group consensus statement and guidelines regarding the current role of imaging techniques in the diagnosis and monitoring of multiple Myeloma. Leukemia. 2009;23(9):1545–1556. - PubMed
-
- Terpos E, Moulopoulos LA, Dimopoulos MA. Advances in imaging and the management of myeloma bone disease. J Clin Oncol. 2011;29(14):1907–1915. - PubMed
-
- Regelink JC, Minnema MC, Terpos E, et al. Comparison of modern and conventional imaging techniques in establishing multiple myeloma-related bone disease: a systematic review. Br J Haematol. 2013;162(1):50–61. - PubMed
-
- Pianko MJ, Terpos E, Roodman GD, et al. Whole-body low-dose computed tomography and advanced imaging techniques for multiple myeloma bone disease. Clin Cancer Res. 2014;20(23):5888–5897. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
