

Association between guideline recommended drugs and death in older adults with multiple chronic conditions: population based cohort study
- PMID: 26432468
- PMCID: PMC4591503
- DOI: 10.1136/bmj.h4984
Association between guideline recommended drugs and death in older adults with multiple chronic conditions: population based cohort study
Abstract
Objective: To estimate the association between guideline recommended drugs and death in older adults with multiple chronic conditions.
Design: Population based cohort study.
Setting: Medicare Current Beneficiary Survey cohort, a nationally representative sample of Americans aged 65 years or more.
Participants: 8578 older adults with two or more study chronic conditions (atrial fibrillation, coronary artery disease, chronic kidney disease, depression, diabetes, heart failure, hyperlipidemia, hypertension, and thromboembolic disease), followed through 2011.
Exposures: Drugs included β blockers, calcium channel blockers, clopidogrel, metformin, renin-angiotensin system (RAS) blockers; selective serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs); statins; thiazides; and warfarin.
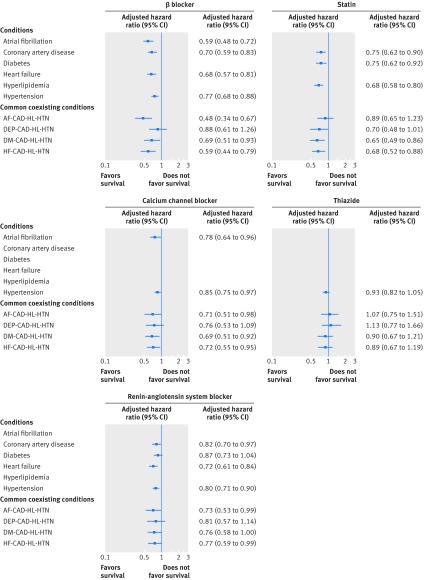
Main outcome measure: Adjusted hazard ratios for death among participants with a condition and taking a guideline recommended drug relative to participants with the condition not taking the drug and among participants with the most common combinations of four conditions.
Results: Over 50% of participants with each condition received the recommended drugs regardless of coexisting conditions; 1287/8578 (15%) participants died during the three years of follow-up. Among cardiovascular drugs, β blockers, calcium channel blockers, RAS blockers, and statins were associated with reduced mortality for indicated conditions. For example, the adjusted hazard ratio for β blockers was 0.59 (95% confidence interval 0.48 to 0.72) for people with atrial fibrillation and 0.68 (0.57 to 0.81) for those with heart failure. The adjusted hazard ratios for cardiovascular drugs were similar to those with common combinations of four coexisting conditions, with trends toward variable effects for β blockers. None of clopidogrel, metformin, or SSRIs/SNRIs was associated with reduced mortality. Warfarin was associated with a reduced risk of death among those with atrial fibrillation (adjusted hazard ratio 0.69, 95% confidence interval 0.56 to 0.85) and thromboembolic disease (0.44, 0.30 to 0.62). Attenuation in the association with reduced risk of death was found with warfarin in participants with some combinations of coexisting conditions.
Conclusions: Average effects on survival, particularly for cardiovascular study drugs, were comparable to those reported in randomized controlled trials but varied for some drugs according to coexisting conditions. Determining treatment effects in combinations of conditions may guide prescribing in people with multiple chronic conditions.
© Tinetti et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Guideline recommended treatments in complex patients with multimorbidity.BMJ. 2015 Oct 2;351:h5145. doi: 10.1136/bmj.h5145. BMJ. 2015. PMID: 26431846 No abstract available.
-
[The guidelines faithful - even in multi-morbid].MMW Fortschr Med. 2015 Nov 5;157(19):35. doi: 10.1007/s15006-015-3724-8. MMW Fortschr Med. 2015. PMID: 26953404 German. No abstract available.
References
-
- Gorina Y, Lentzer H. Multiple causes of death in old age. Aging Trends 2008;(9):1-9. - PubMed
-
- National Center for Health Statistics. Mortality data, multiple-cause-of-death public-use data files. 2015. www.cdc.gov/nchs/data_access/VitalStatsOnline.htm#Mortality_Multiple.
-
- Hoyert DL, Xu JQ. Deaths: preliminary data for 2011. National Vital Statistics Reports; Vol 61 No 6. National Center for Health Statistics; 2012. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical