

Obstructive airway in Morquio A syndrome, the past, the present and the future
- PMID: 26432669
- PMCID: PMC4755902
- DOI: 10.1016/j.ymgme.2015.09.007
Obstructive airway in Morquio A syndrome, the past, the present and the future
Abstract
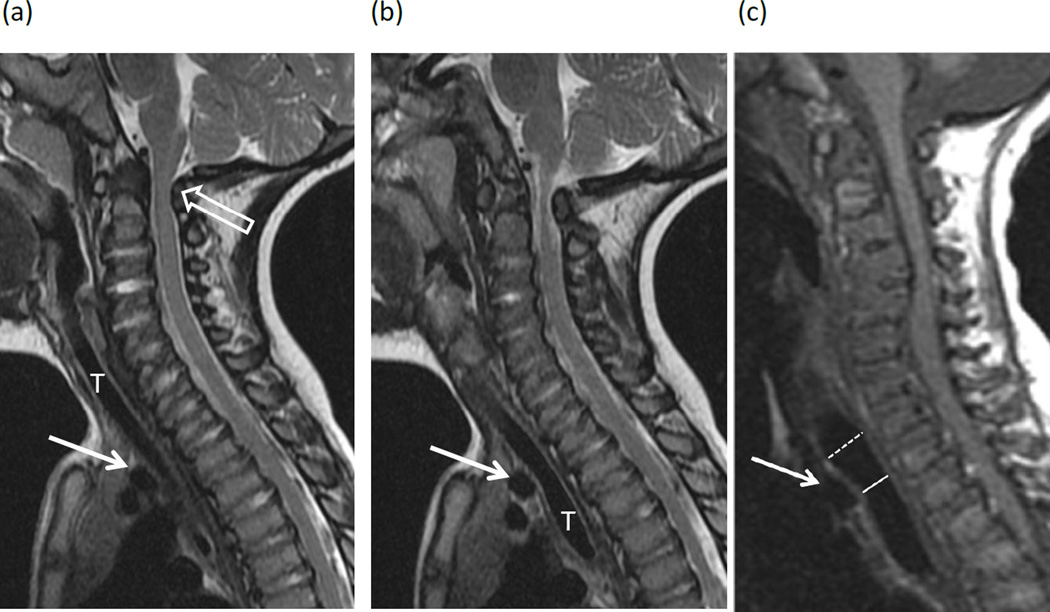
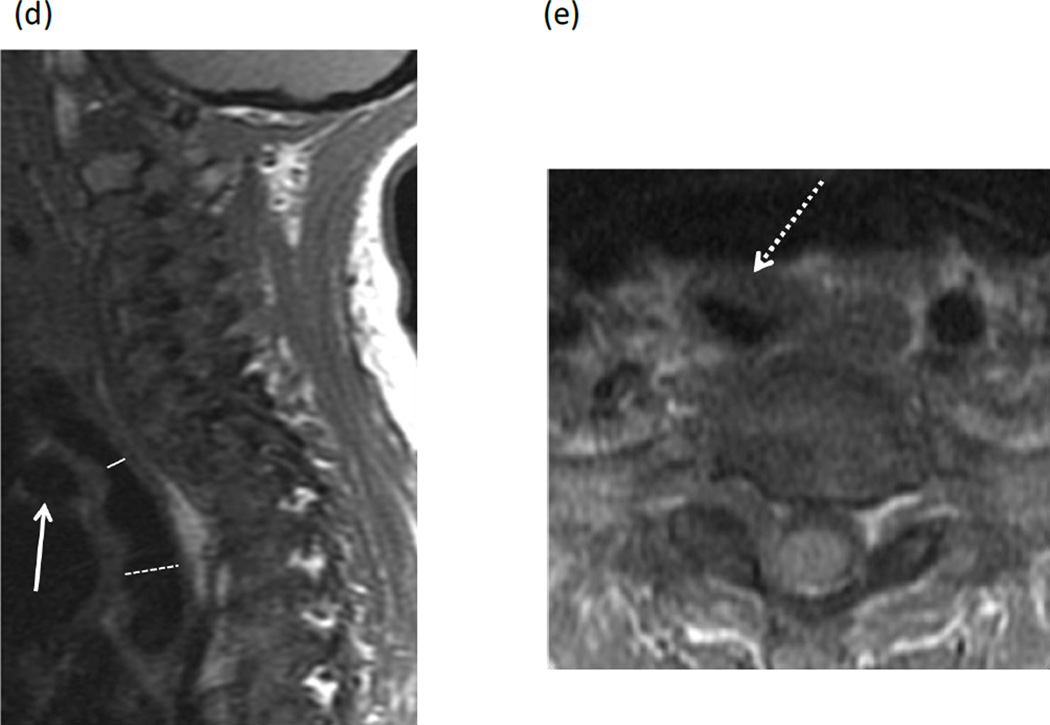
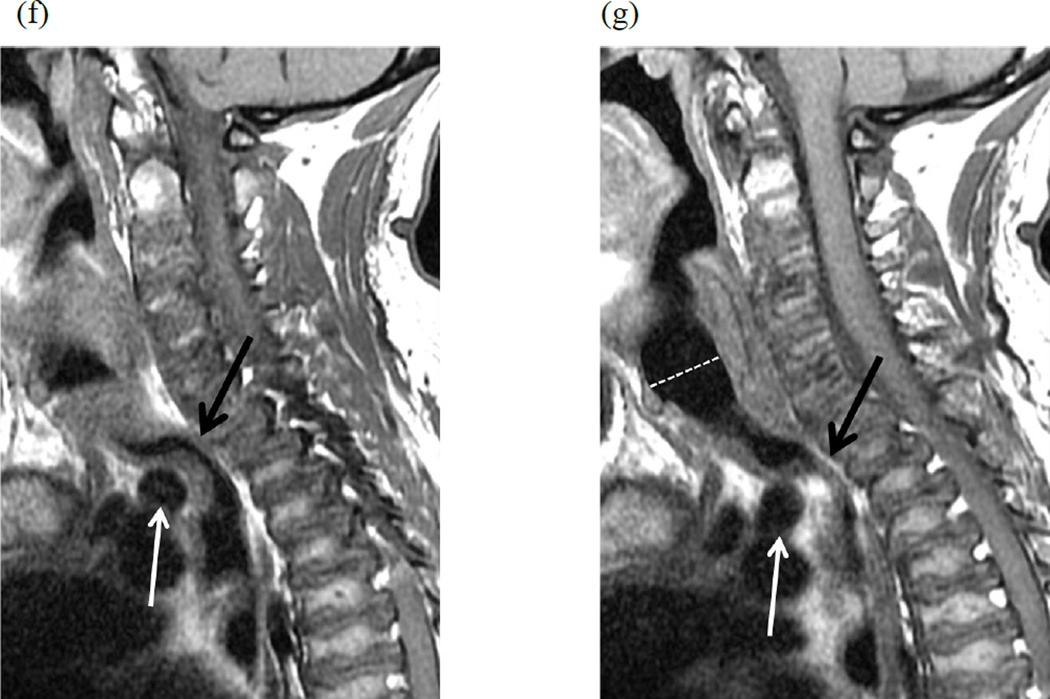
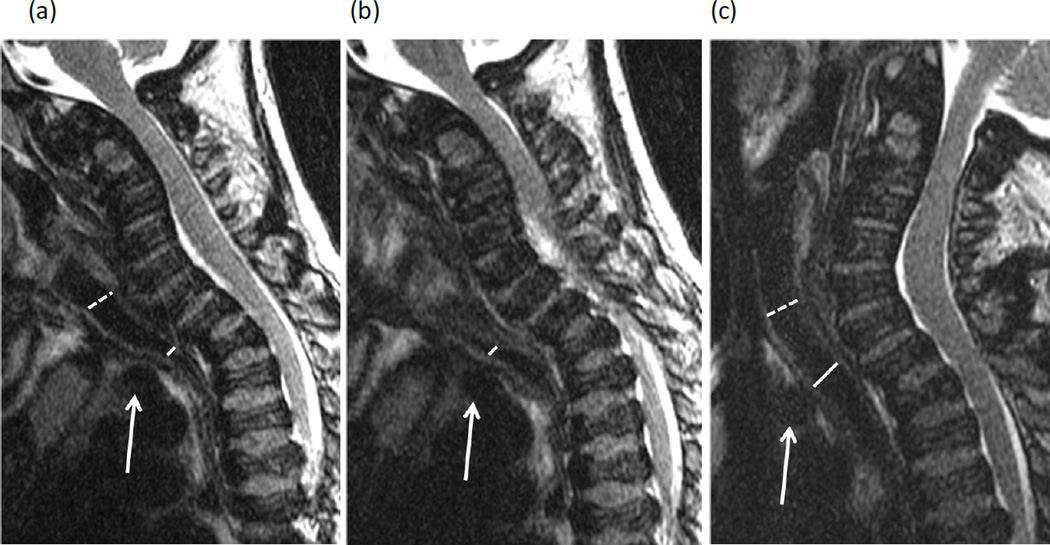
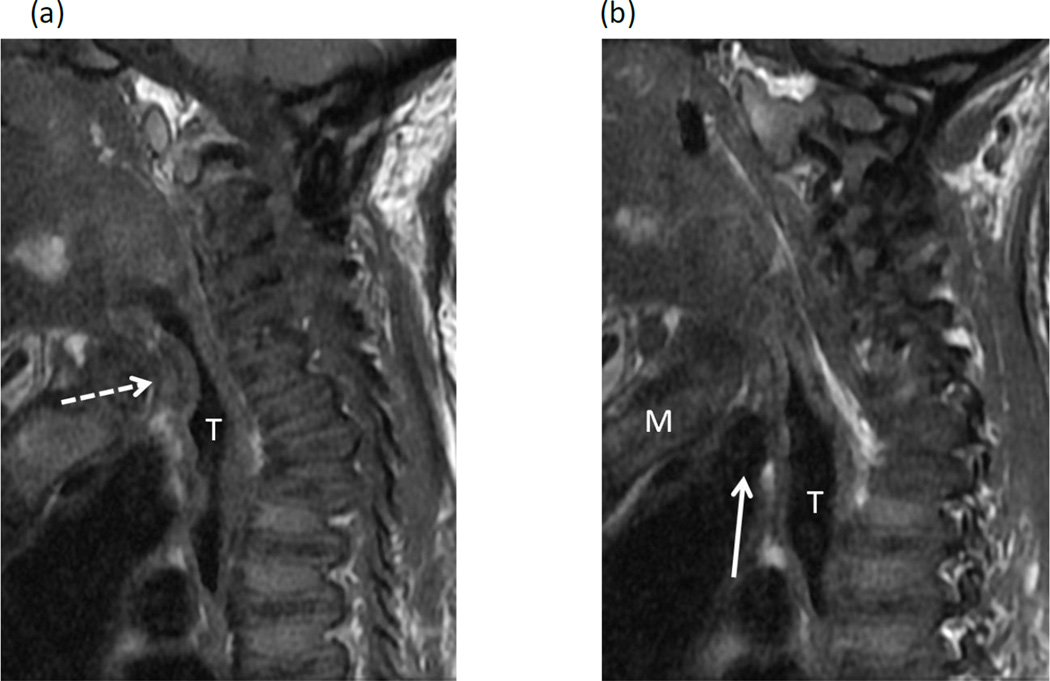
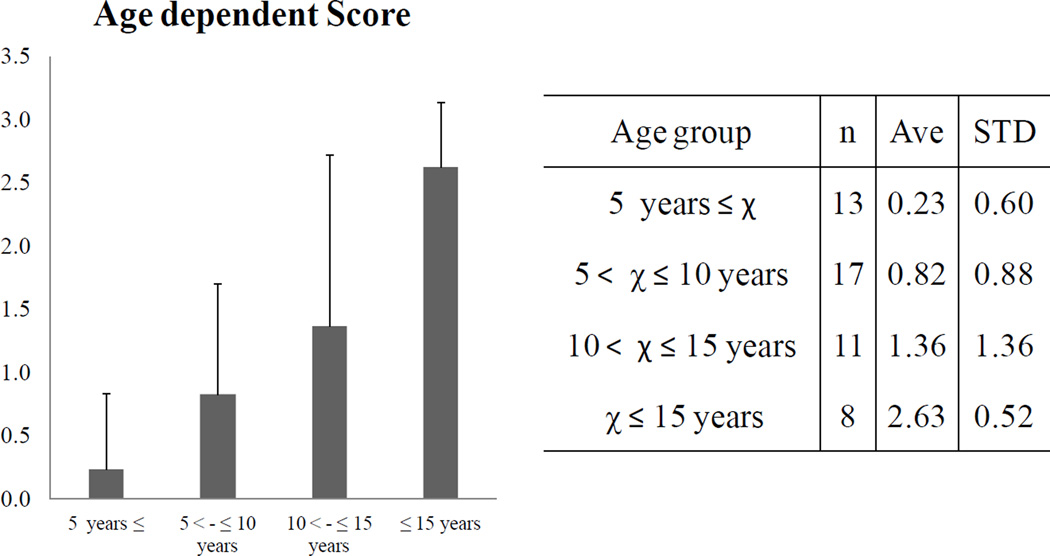
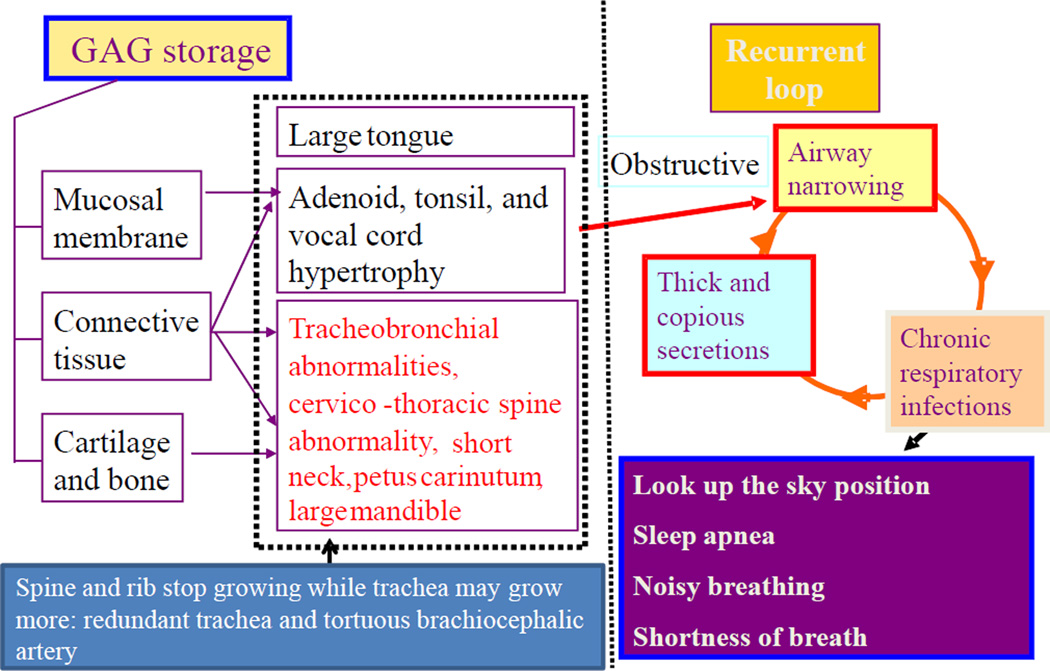
Patients with severe tracheal obstruction in Morquio A syndrome are at risk of dying of sleep apnea and related complications. Tracheal obstruction also leads to life-threatening complications during anesthesia as a result of the difficulty in managing the upper airway due to factors inherent to the Morquio A syndrome, compounded by the difficulty in intubating the trachea. A detailed description of the obstructive pathology of the trachea is not available in the literature probably due to lack of a homogenous group of Morquio A patients to study at any one particular center. We present a series of cases with significant tracheal obstruction who were unrecognized due to the difficulty in interpreting tracheal narrowing airway symptoms. Our goal is to provide the guidelines in the management of these patients that allow earlier recognition and intervention of tracheal obstruction. Sagittal MRI images of the cervical spine of 28 Morquio A patients (12±8.14years) showed that19/28 (67.9%) patients had at least 25% tracheal narrowing and that narrowing worsened with age (all 8 patients over 15years had greater than 50% narrowing). Eight out of 28 patients were categorized as severe (>75%) tracheal narrowing when images were evaluated in neutral head and neck position. Of the 19 patients with tracheal narrowing, compression by the tortuous brachiocephalic artery was the most common cause (n=15). Evidence of such tracheal narrowing was evident as early as at 2years of age. The etiology of tracheal impingement by the brachiocephalic artery in Morquio A appears to be due to a combination of the narrow thoracic inlet crowding structures and the disproportionate growth of trachea and brachiocephalic artery in relationship to the chest cavity leading to tracheal tortuosity. In conclusion, tracheal narrowing, often due to impression from the crossing tortuous brachiocephalic artery, increases with age in Morquio A patients. Greater attention to the trachea is needed when evaluating cervical spine MRIs as well as other imaging and clinical investigations, with the goal of establishing a timely treatment protocol to reduce the mortality rate in this patient population.
Keywords: Brachiocephalic artery; Disproportionate growth; MRI; Morquio A syndrome; Tracheal obstruction.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
All the authors contributed to the Article and had no conflict of interest with any other party.
Shunji Tomatsu, Lauren W. Averill, Kazuki Sawamoto, William G. Mackenzie, Michael B. Bober, Christian Pizarro, Christopher J. Goff, Li Xie, Tadao Orii, and Mary Theroux declare that they have no conflict of interests.
Figures
References
-
- Morquio L. Sur une forme de dystrophie osseuse familial. Archives de médicine des infants, Paris. 1929;32:129–135.
-
- Neufeld EF, Muenzer J. The mucopolysaccharidoses. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The Metabolic and Molecular Bases of inherited Disease. 8th ed. New York: McGraw-Hill; 2001. pp. 3421–3452.
-
- Tomatsu S, Montaño AM, Oikawa H, et al. Handbook of Growth and Growth Monitoring in Health and Disease 1. New York: Springer; 2012. Impairment of Body Growth in Mucopolysaccharidoses; pp. 2091–2117.
-
- Tomatsu S, Montaño AM, Oikawa H, et al. Mucopolysaccharidosis type IVA (Morquio A disease): clinical review and current treatment. Cur Pharm Biotech. 2011;12:931–945. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
