

Multimorbidity, Depression, and Mortality in Primary Care: Randomized Clinical Trial of an Evidence-Based Depression Care Management Program on Mortality Risk
- PMID: 26432693
- PMCID: PMC4803701
- DOI: 10.1007/s11606-015-3524-y
Multimorbidity, Depression, and Mortality in Primary Care: Randomized Clinical Trial of an Evidence-Based Depression Care Management Program on Mortality Risk
Abstract
Background: Two-thirds of older adults have two or more medical conditions that often take precedence over depression in primary care.
Objective: We evaluated whether evidence-based depression care management would improve the long-term mortality risk among older adults with increasing levels of medical comorbidity.
Design: Longitudinal analyses of the practice-randomized Prevention of Suicide in Primary Care Elderly: Collaborative Trial (PROSPECT). Twenty primary care practices randomized to intervention or usual care.
Patients: The sample included 1204 older primary care patients completing the Charlson Comorbidity Index (CCI) and other interview questions at baseline.
Intervention: For 2 years, a depression care manager worked with primary care physicians to provide algorithm-based care for depression, offering psychotherapy, increasing the antidepressant dose if indicated, and monitoring symptoms, medication adverse effects, and treatment adherence.
Main measures: Depression status based on clinical interview, CCI to evaluate medical comorbidity, and vital status at 8 years (National Death Index).
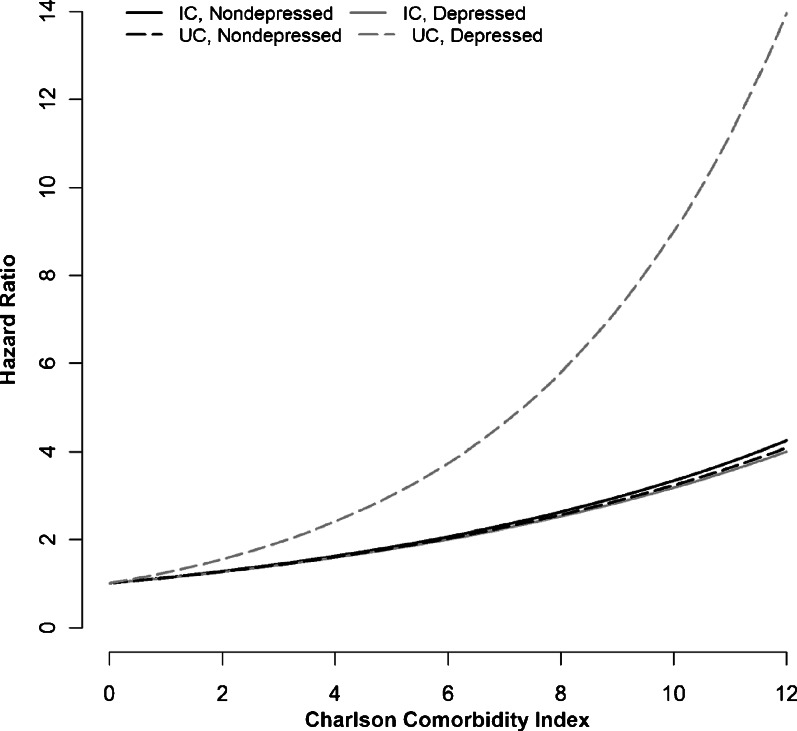
Key results: In the usual care condition, patients with the highest levels of medical comorbidity and depression were at increased risk of mortality over the course of the follow-up compared to depressed patients with minimal medical comorbidity [hazard ratio 3.02 (95% CI, 1.32 to 8.72)]. In contrast, in intervention practices, patients with the highest level of medical comorbidity and depression compared to depressed patients with minimal medical comorbidity were not at significantly increased risk [hazard ratio 1.73 (95% CI, 0.86 to 3.96)]. Nondepressed patients in intervention and usual care practices had similar mortality risk.
Conclusions: Depression management mitigated the combined effect of multimorbidity and depression on mortality. Depression management should be integral to optimal patient care, not a secondary focus.
Trial registration: ClinicalTrials.gov NCT00000367.
Figures
Comment in
-
Capsule Commentary on Gallo et al., Multimorbidity, Depression, and Mortality in Primary Care: Randomized Clinical Trial of an Evidence-Based Depression Care Management Program on Mortality Risk.J Gen Intern Med. 2016 Apr;31(4):412. doi: 10.1007/s11606-016-3589-2. J Gen Intern Med. 2016. PMID: 26857728 Free PMC article. No abstract available.
References
-
- Smith SM, Soubhi H, Fortin M, Hudon C, O'Dowd T. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2012;4:CD006560. - PubMed
-
- Mezuk B, Gallo JJ. Depression and medical illness in late life: Race, resources, and stress. In: Lavretsky H, Sajatovic M, Reynolds CF, editors. Depression in Late Life. London: Oxford University Press; 2013. pp. 270–94.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
