

Economic and epidemiological impact of early antiretroviral therapy initiation in India
- PMID: 26434780
- PMCID: PMC4592848
- DOI: 10.7448/IAS.18.1.20217
Economic and epidemiological impact of early antiretroviral therapy initiation in India
Abstract
Introduction: Recent WHO guidance advocates for early antiretroviral therapy (ART) initiation at higher CD4 counts to improve survival and reduce HIV transmission. We sought to quantify how the cost-effectiveness and epidemiological impact of early ART strategies in India are affected by attrition throughout the HIV care continuum.
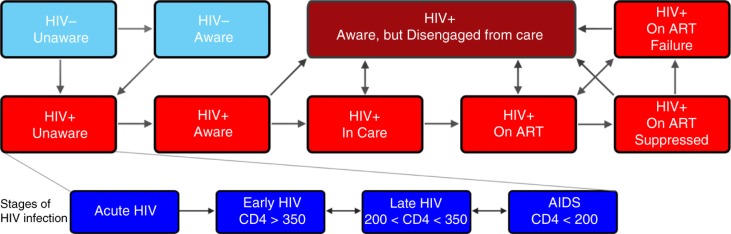
Methods: We constructed a dynamic compartmental model replicating HIV transmission, disease progression and health system engagement among Indian adults. Our model of the Indian HIV epidemic compared implementation of early ART initiation (i.e. initiation above CD4 ≥350 cells/mm(3)) with delayed initiation at CD4 ≤350 cells/mm(3); primary outcomes were incident cases, deaths, quality-adjusted-life-years (QALYs) and costs over 20 years. We assessed how costs and effects of early ART initiation were impacted by suboptimal engagement at each stage in the HIV care continuum.
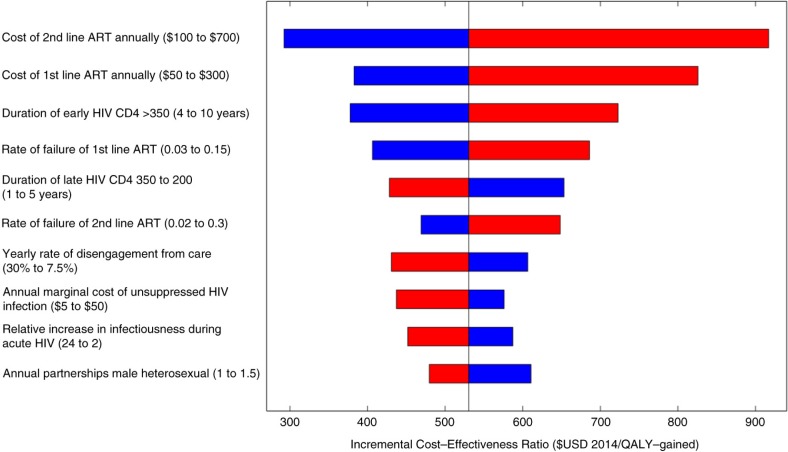
Results: Assuming "idealistic" engagement in HIV care, early ART initiation is highly cost-effective ($442/QALY-gained) compared to delayed initiation at CD4 ≤350 cells/mm(3) and could reduce new HIV infections to <15,000 per year within 20 years. However, when accounting for realistic gaps in care, early ART initiation loses nearly half of potential epidemiological benefits and is less cost-effective ($530/QALY-gained). We project 1,285,000 new HIV infections and 973,000 AIDS-related deaths with deferred ART initiation with current levels of care-engagement in India. Early ART initiation in this continuum resulted in 1,050,000 new HIV infections and 883,000 AIDS-related deaths, or 18% and 9% reductions (respectively), compared to current guidelines. Strengthening HIV screening increases benefits of earlier treatment modestly (1,001,000 new infections; 22% reduction), while improving retention in care has a larger modulatory impact (676,000 new infections; 47% reduction).
Conclusions: Early ART initiation is highly cost-effective in India but only has modest epidemiological benefits at current levels of care-engagement. Improved retention in care is needed to realize the full potential of earlier treatment.
Keywords: HIV; India; antiretroviral therapy; continuum of care; cost-effectiveness.
Figures

Comment in
-
Cost-effectiveness analysis of 'test and treat' policy for antiretroviral therapy among heterosexual HIV population in India.Indian J Med Res. 2022 Jun;156(6):705-714. doi: 10.4103/ijmr.IJMR_806_20. Indian J Med Res. 2022. PMID: 37056069 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS) UNAIDS Gap Report 2014; Geneva: UNAIDS; 2014. - PubMed
-
- Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, Wabwire-Mangen F, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. N Engl J Med. 2000;342(13):921–9. Rakai Project Study Group. - PubMed
-
- Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373(9657):48–57. - PubMed
-
- World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infections: recommendations for a public health approach. Geneva: WHO; 2013. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
