

Endometriosis diagnosis and staging by operating surgeon and expert review using multiple diagnostic tools: an inter-rater agreement study
- PMID: 26435386
- PMCID: PMC4821828
- DOI: 10.1111/1471-0528.13711
Endometriosis diagnosis and staging by operating surgeon and expert review using multiple diagnostic tools: an inter-rater agreement study
Abstract
Objective: To determine agreement on endometriosis diagnosis between real-time laparoscopy and subsequent expert review of digital images, operative reports, magnetic resonance imaging (MRI), and histopathology, viewed sequentially.
Design: Inter-rater agreement study.
Setting: Five urban surgical centres.
Population: Women, aged 18-44 years, who underwent a laparoscopy regardless of clinical indication. A random sample of 105 women with and 43 women without a postoperative endometriosis diagnosis was obtained from the ENDO study.
Methods: Laparoscopies were diagnosed, digitally recorded, and reassessed.
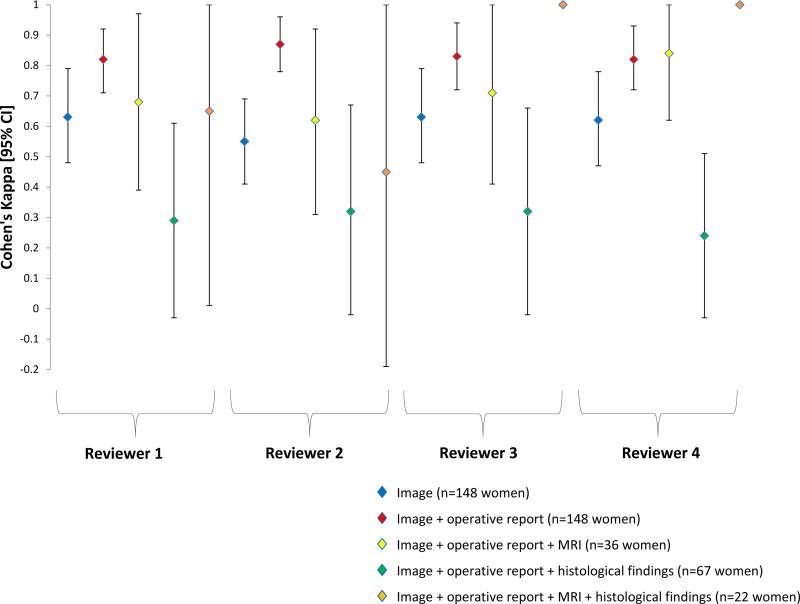
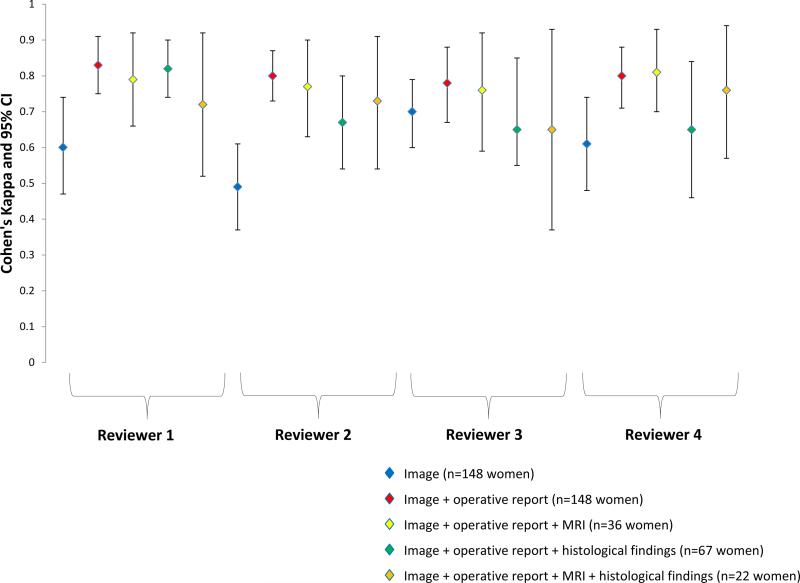
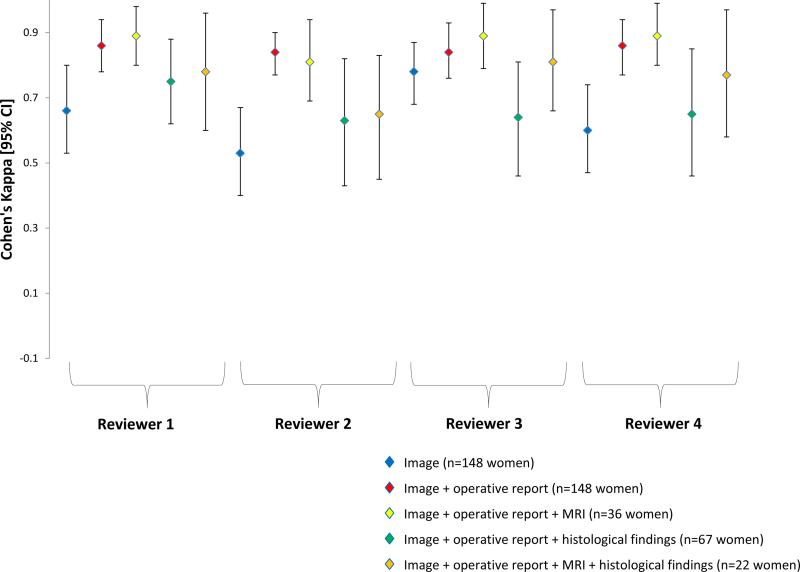
Main outcome measures: Inter-observer agreement of endometriosis diagnosis and staging according to the revised American Society for Reproductive Medicine criteria. Prevalence and bias-adjusted kappa values (κ) were calculated for diagnosis, and weighted κ values were calculated for staging.
Results: Surgeons and expert reviewers had substantial agreement on diagnosis and staging after viewing digital images (n = 148; mean κ = 0.67, range 0.61-0.69; mean κ = 0.64, range 0.53-0.78, respectively) and after additionally viewing operative reports (n = 148; mean κ = 0.88, range 0.85-0.89; mean κ = 0.85, range 0.84-0.86, respectively). Although additionally viewing MRI findings (n = 36) did not greatly impact agreement, agreement substantially decreased after viewing histological findings (n = 67), with expert reviewers changing their assessment from a positive to a negative diagnosis in up to 20% of cases.
Conclusion: Although these findings suggest that misclassification bias in the diagnosis or staging of endometriosis via visualised disease is minimal, they should alert gynaecologists who review operative images in order to make decisions on endometriosis treatment that operative reports/drawings and histopathology, but not necessarily MRI, will improve their ability to make sound judgments.
Tweetable abstract: Endometriosis diagnosis and staging agreement between expert reviewers and operating surgeons was substantial.
Keywords: Endometriosis; epidemiology; histology; laparoscopy; magnetic resonance imaging; reliability.
© 2015 Royal College of Obstetricians and Gynaecologists.
Figures
Comment in
-
Visual endometriosis diagnosis is reliable but outpatient tests needed.BJOG. 2017 Jan;124(2):230. doi: 10.1111/1471-0528.13854. Epub 2016 Feb 1. BJOG. 2017. PMID: 28012268 No abstract available.
References
-
- Rawson JM. Prevalence of endometriosis in asymptomatic women. J Reprod Med. 1991;36:513–515. - PubMed
-
- Balasch J, Creus M, Fábregues F, Carmona F, Ordi J, Martinez-Román S, et al. Visible and non-visible endometriosis at laparoscopy in fertile and infertile women and in patients with chronic pelvic pain: a prospective study. Hum Reprod. 1996;11:387–391. - PubMed
-
- Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet Gynecol Clin North Am. 1997;24:235–258. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
