

Chewing-induced hypertension in afferent baroreflex failure: a sympathetic response?
- PMID: 26435473
- PMCID: PMC5074388
- DOI: 10.1113/EP085340
Chewing-induced hypertension in afferent baroreflex failure: a sympathetic response?
Abstract
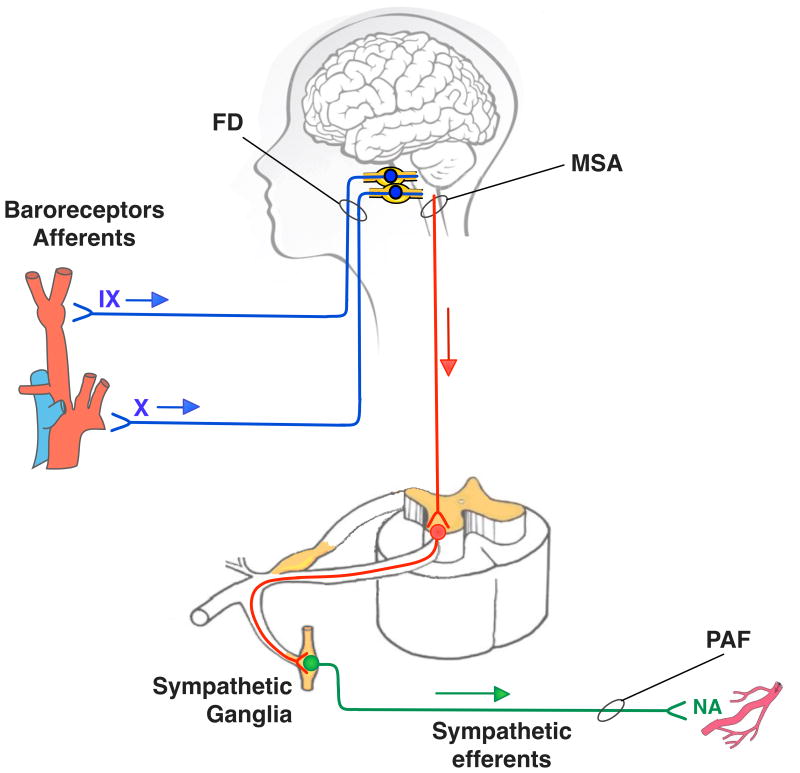
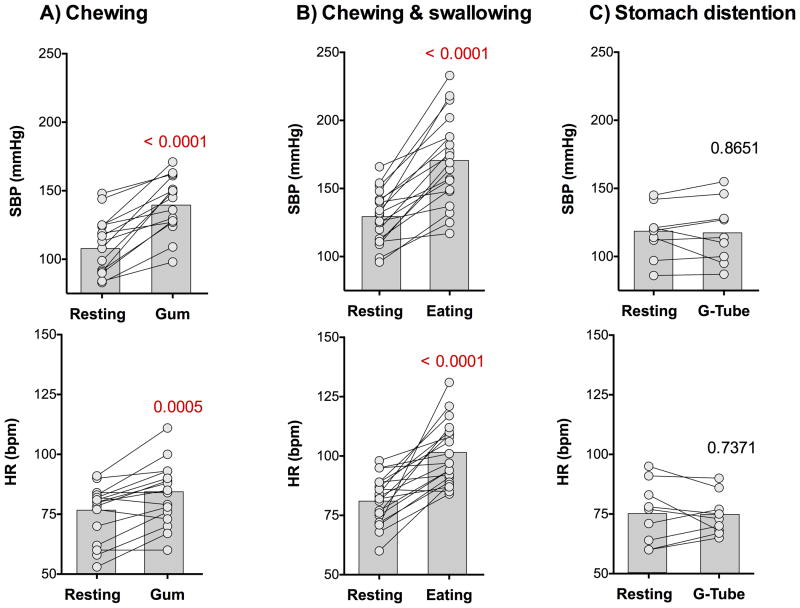
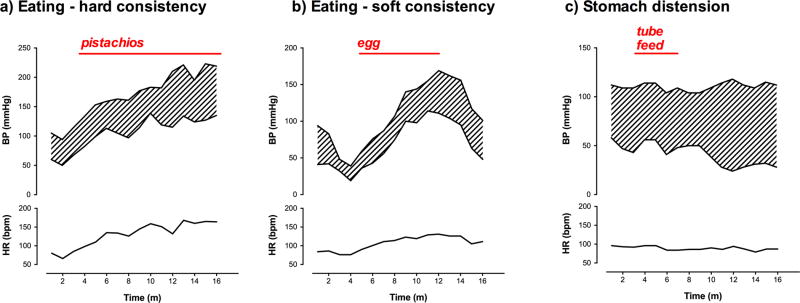
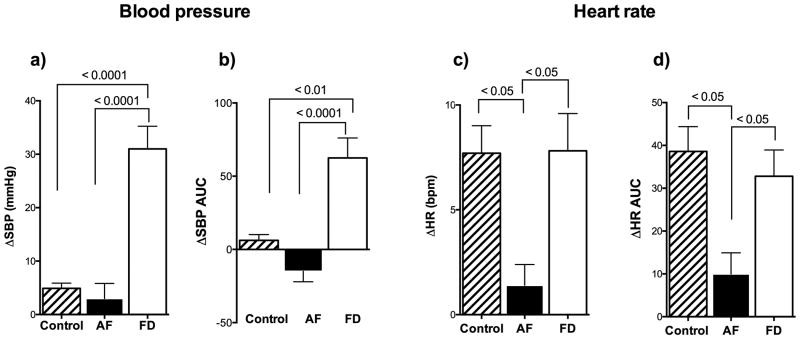
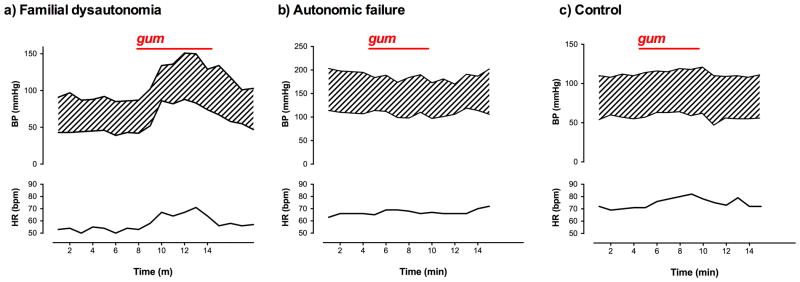
What is the central question of this study? Our goal was to understand the autonomic responses to eating in patients with congenital afferent baroreflex failure, by documenting changes in blood pressure and heart rate with chewing, swallowing and stomach distension. What is the main finding and its importance? Patients born with lesions in the afferent baroreceptor pathways have an exaggerated pressor response to food intake. This appears to be a sympathetically mediated response, triggered by chewing, that occurs independently of swallowing or distension of the stomach. The chewing-induced pressor response may be useful as a counter-manoeuvre to prevent orthostatic hypotension in these patients. Familial dysautonomia (FD) is a rare genetic disease with extremely labile blood pressure resulting from baroreflex deafferentation. Patients have marked surges in sympathetic activity, frequently surrounding meals. We conducted an observational study to document the autonomic responses to eating in patients with FD and to determine whether sympathetic activation was caused by chewing, swallowing or stomach distension. Blood pressure and R-R intervals were measured continuously while chewing gum (n = 15), eating (n = 20) and distending the stomach by percutaneous endoscopic gastrostomy tube feeding (n = 9). Responses were compared with those of normal control subjects (n = 10) and of patients with efferent autonomic failure (n = 10) who have chronically impaired sympathetic outflow. In patients with FD, eating was associated with a marked but transient pressor response (P < 0.0001) and additional signs of sympathetic activation, including tachycardia, diaphoresis and flushing of the skin. Chewing gum evoked a similar increase in blood pressure that was higher in patients with FD than in control subjects (P = 0.0001), but was absent in patients with autonomic failure. In patients with FD, distending the stomach by percutaneous endoscopic gastrostomy tube feeding failed to elicit a pressor response. The results provide indirect evidence that chewing triggers sympathetic activation. The increase in blood pressure is exaggerated in patients with FD as a result of blunted afferent baroreceptor signalling. The chewing pressor response may be useful as a counter-manoeuvre to raise blood pressure and prevent symptomatic orthostatic hypotension in patients with FD.
© 2015 The Authors. Experimental Physiology © 2015 The Physiological Society.
Conflict of interest statement
There are no conflicts of interest
Figures

References
-
- Abe N, Yashiro K, Hidaka O, Takada K. Influence of gum-chewing on the haemodynamics in female masseter muscle. Journal of Oral Rehabilitation. 2009;36:240–249. - PubMed
-
- Aguayo AJ, Nair CP, Bray GM. Peripheral nerve abnormalities in the Riley-Day syndrome. Findings in a sural nerve biopsy. Arch Neurol. 1971;24:106–116. - PubMed
-
- Axelrod FB, Goldberg JD, Ye XY, Maayan C. Survival in familial dysautonomia: Impact of early intervention. J Pediatr. 2002;141:518–523. - PubMed
-
- Axelrod FB, Gouge TH, Ginsburg HB, Bangaru BS, Hazzi C. Fundoplication and gastrostomy in familial dysautonomia. J Pediatr. 1991;118:388–394. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical