

Identifying osteoporotic vertebral fracture
- PMID: 26435923
- PMCID: PMC4559972
- DOI: 10.3978/j.issn.2223-4292.2015.08.01
Identifying osteoporotic vertebral fracture
Abstract
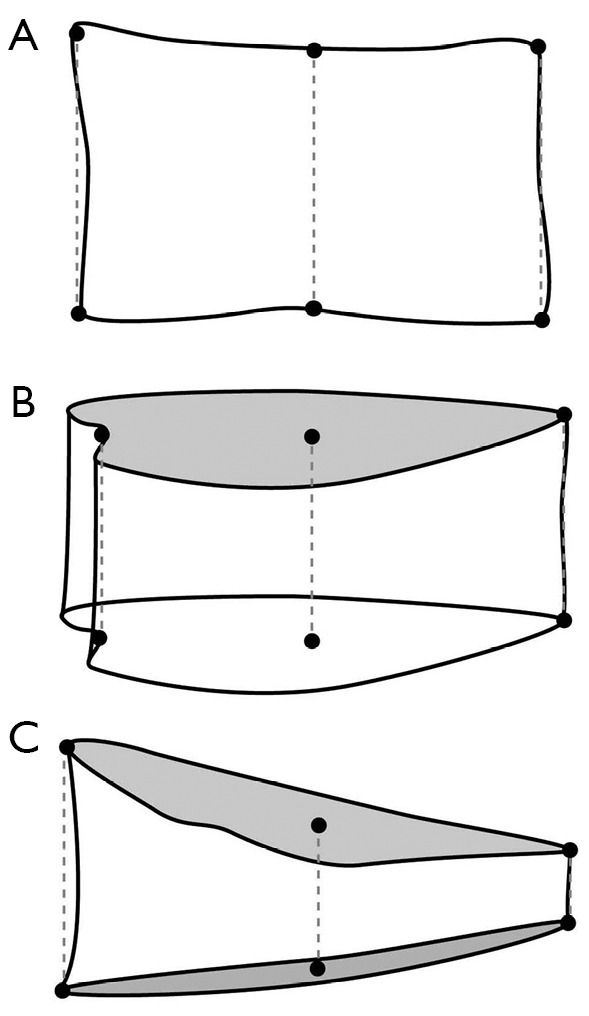
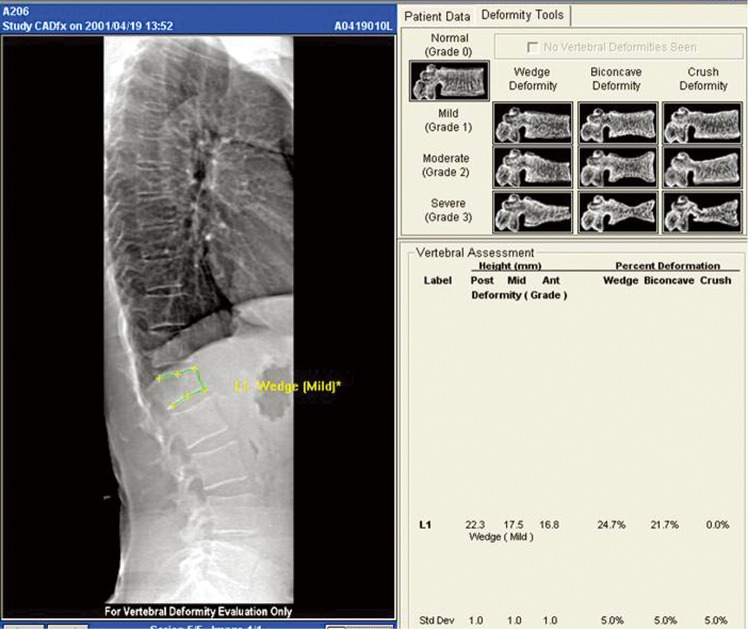
Osteoporosis per se is not a harmful disease. It is the sequela of osteoporosis and most particularly the occurrence of osteoporotic fracture that makes osteoporosis a serious medical condition. All of the preventative measures, investigations, treatment and research into osteoporosis have one primary goal and that is to prevent the occurrence of osteoporotic fracture. Vertebral fracture is by far and away the most prevalent osteoporotic fracture. The significance and diagnosis of vertebral fracture are discussed in this article.
Keywords: Vertebral fracture; computed tomography (CT); magnetic resonance imaging (MRI); metastases; osteoporosis; radiography.
Conflict of interest statement
Figures

References
-
- Cooper C, Atkinson EJ, O'Fallon WM, Melton LJ, 3rd. Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985-1989. J Bone Miner Res 1992;7:221-7. - PubMed
-
- Lips P, van Schoor NM. Quality of life in patients with osteoporosis. Osteoporos Int 2005;16:447-55. - PubMed
-
- Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR. Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 1999;159:1215-20. - PubMed
-
- Siris ES, Miller PD, Barrett-Connor E, Faulkner KG, Wehren LE, Abbott TA, Berger ML, Santora AC, Sherwood LM. Identification and fracture outcomes of undiagnosed low bone mineral density in postmenopausal women: results from the National Osteoporosis Risk Assessment. JAMA 2001;286:2815-22. - PubMed
Publication types
LinkOut - more resources
Full Text Sources