

Short and tall stature: a new paradigm emerges
- PMID: 26437621
- PMCID: PMC5002943
- DOI: 10.1038/nrendo.2015.165
Short and tall stature: a new paradigm emerges
Abstract
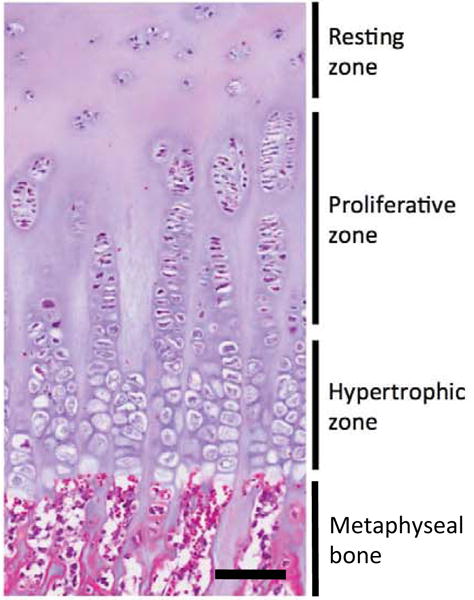
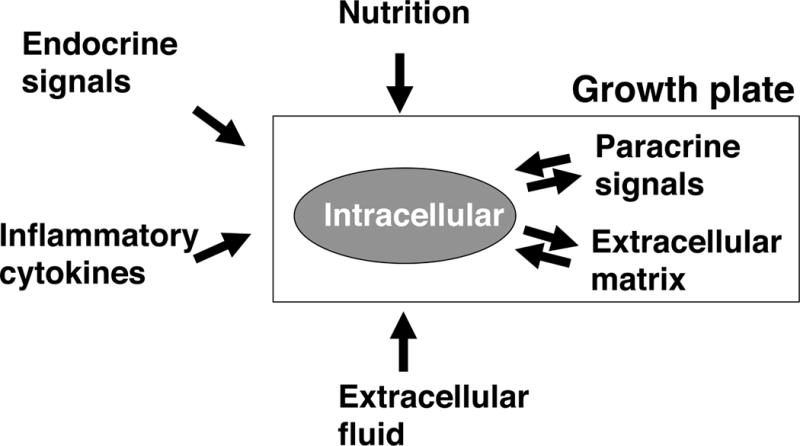
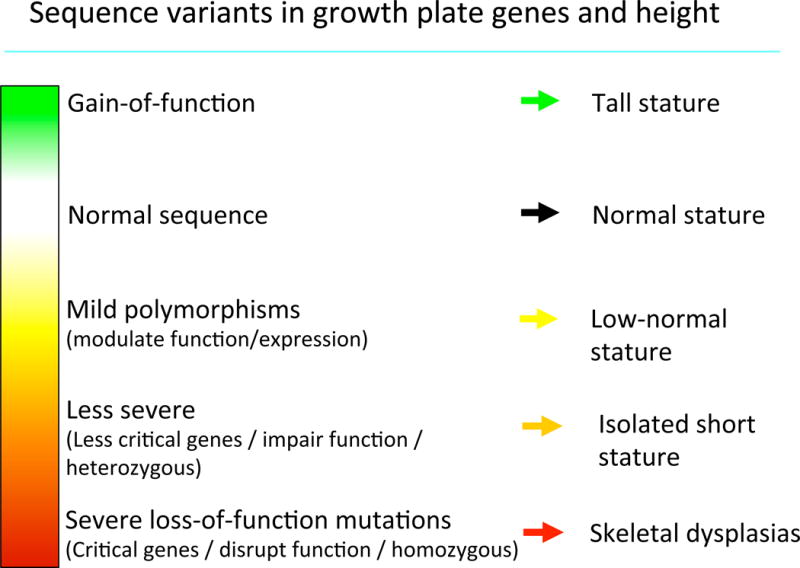
In the past, the growth hormone (GH)-insulin-like growth factor 1 (IGF-1) axis was often considered to be the main system that regulated childhood growth and, therefore, determined short stature and tall stature. However, findings have now revealed that the GH-IGF-1 axis is just one of many regulatory systems that control chondrogenesis in the growth plate, which is the biological process that drives height gain. Consequently, normal growth in children depends not only on GH and IGF-1 but also on multiple hormones, paracrine factors, extracellular matrix molecules and intracellular proteins that regulate the activity of growth plate chondrocytes. Mutations in the genes that encode many of these local proteins cause short stature or tall stature. Similarly, genome-wide association studies have revealed that the normal variation in height seems to be largely due to genes outside the GH-IGF-1 axis that affect growth at the growth plate through a wide variety of mechanisms. These findings point to a new conceptual framework for understanding short and tall stature that is centred not on two particular hormones but rather on the growth plate, which is the structure responsible for height gain.
Conflict of interest statement
Declaration of interests FDL, and JMW have no interests to declare. JB is listed as a co-inventor on a patent application by the National Institutes of Health for targeted treatment of cartilage disorders. LS has received speakers’ honoraria and/or research support from Novo Nordisk, Pfizer, Ferring, and Merck Serono and has submitted a patent application for novel peptides to treat bone or cartilage disorders and other diseases. AD has been a faculty speaker at continuing medical education symposia sponsored by Novo Nordisk, Sandoz, and Ipsen. MP has received research support from Novo Nordisk, Pfizer, Teva, personal fees from Novo Nordisk, and is a director of NG Solutions Ltd. ON has received an ESPE research fellowship sponsored by Novo Nordisk and speaker’s honorarium from Lilly.
Figures
References
-
- Daughaday WH. Growth hormone axis overview–somatomedin hypothesis. Pediatr Nephrol. 2000;14(7):537–40. - PubMed
-
- Roth J, Glick SM, Yalow RS, Berson SA. The Influence of Blood Glucose on the Plasma Concentration of Growth Hormone. Diabetes. 1964;13:355–61. - PubMed
-
- Melmed S, Williams RH, Larsen PR, Kronenberg H. Williams textbook of endocrinology. 12th. Philadelphia: Elsevier/Saunders; 2011.
-
- Rosenfeld RG. The molecular basis of idiopathic short stature. Growth Horm IGF Res. 2005;15(Suppl A):S3–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
