

Endovascular Recanalization Therapy in Acute Ischemic Stroke: Updated Meta-analysis of Randomized Controlled Trials
- PMID: 26437993
- PMCID: PMC4635708
- DOI: 10.5853/jos.2015.17.3.268
Endovascular Recanalization Therapy in Acute Ischemic Stroke: Updated Meta-analysis of Randomized Controlled Trials
Abstract
Background and purpose: Recent randomized clinical trials (RCTs) have demonstrated benefits of endovascular recanalization therapy (ERT) contrary to earlier trials. We aimed to estimate the benefits of ERT added to standard therapy in acute ischemic stroke.
Methods: From a literature search of RCTs testing ERT, we performed a meta-analysis to estimate an overall efficacy and safety of ERT for all trials, stent-retriever trials, and RCTs comparing ERT and intravenous tissue plasminogen activator (IV-TPA).
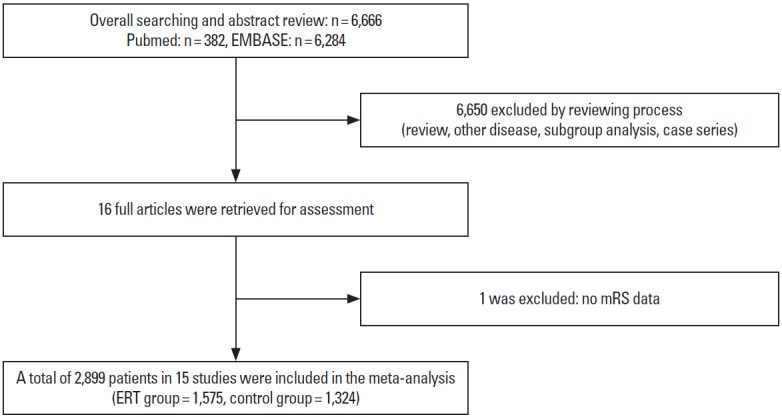
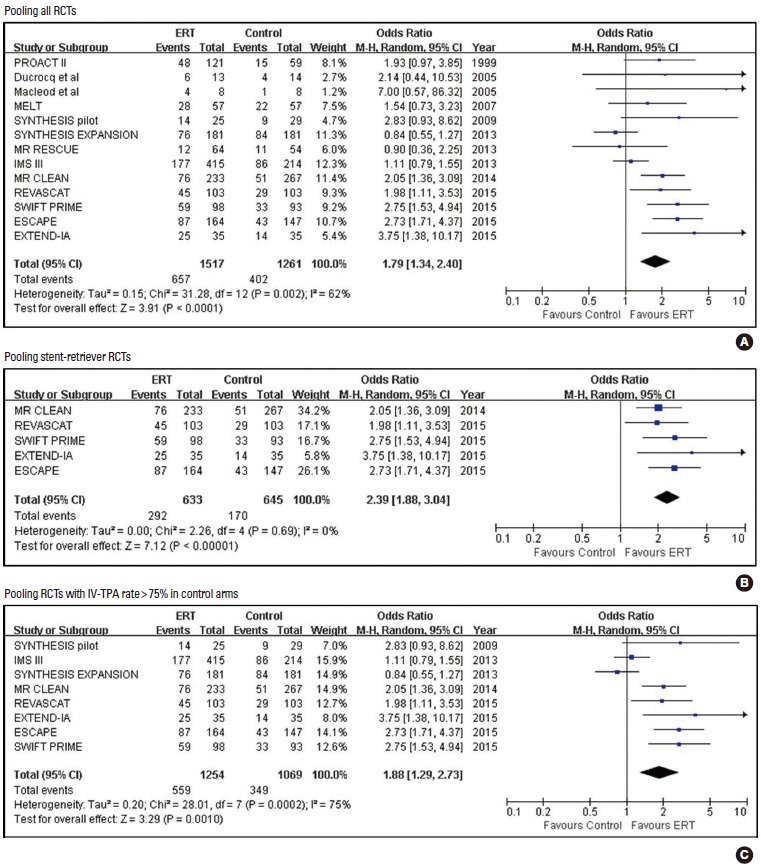
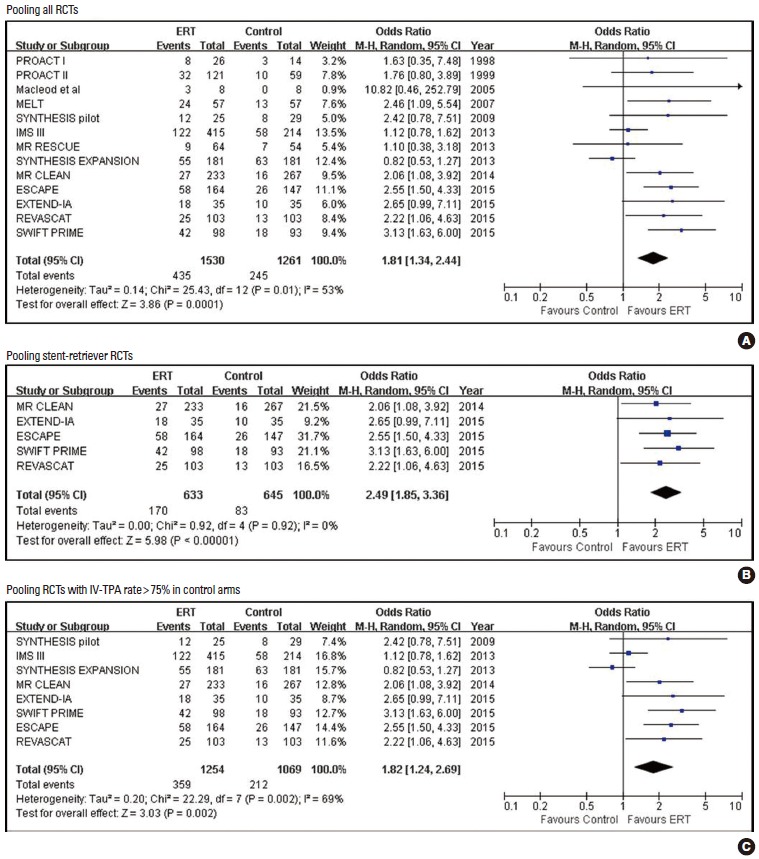
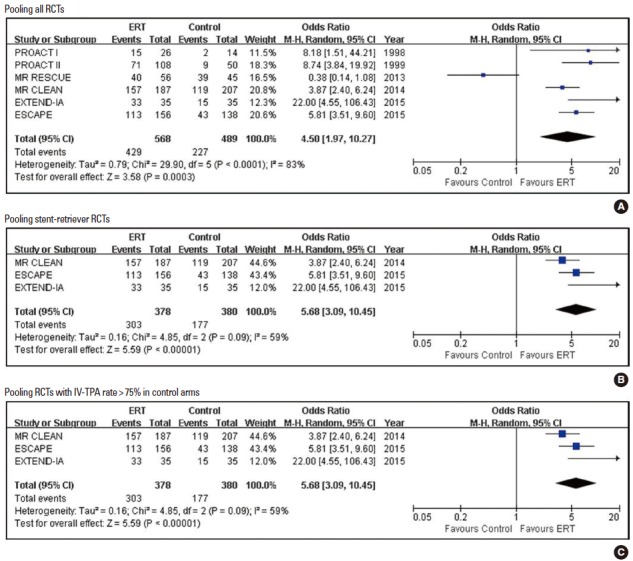
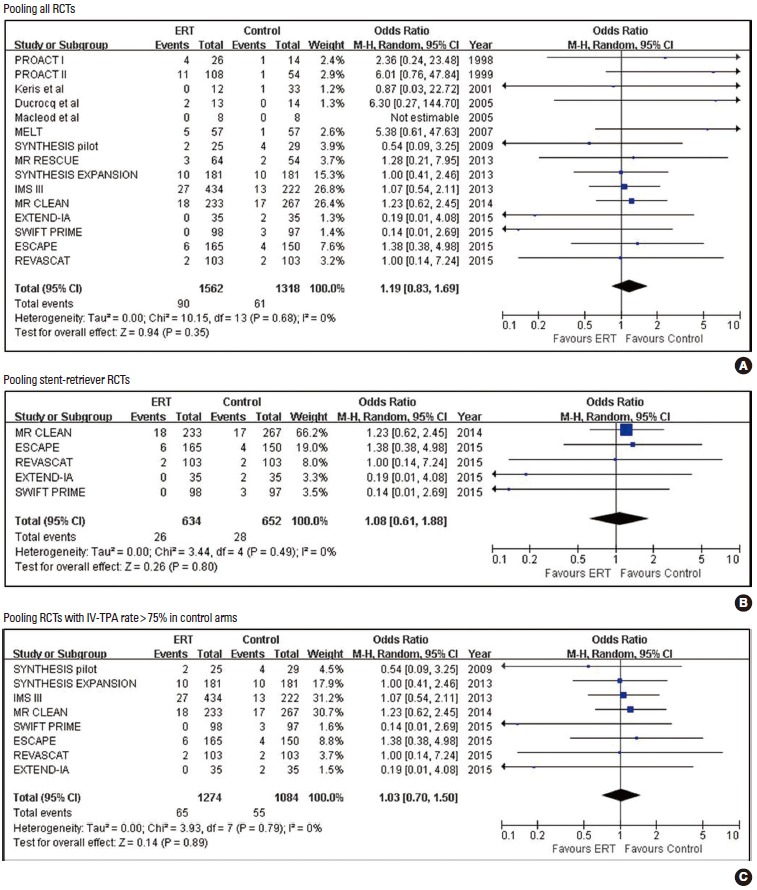
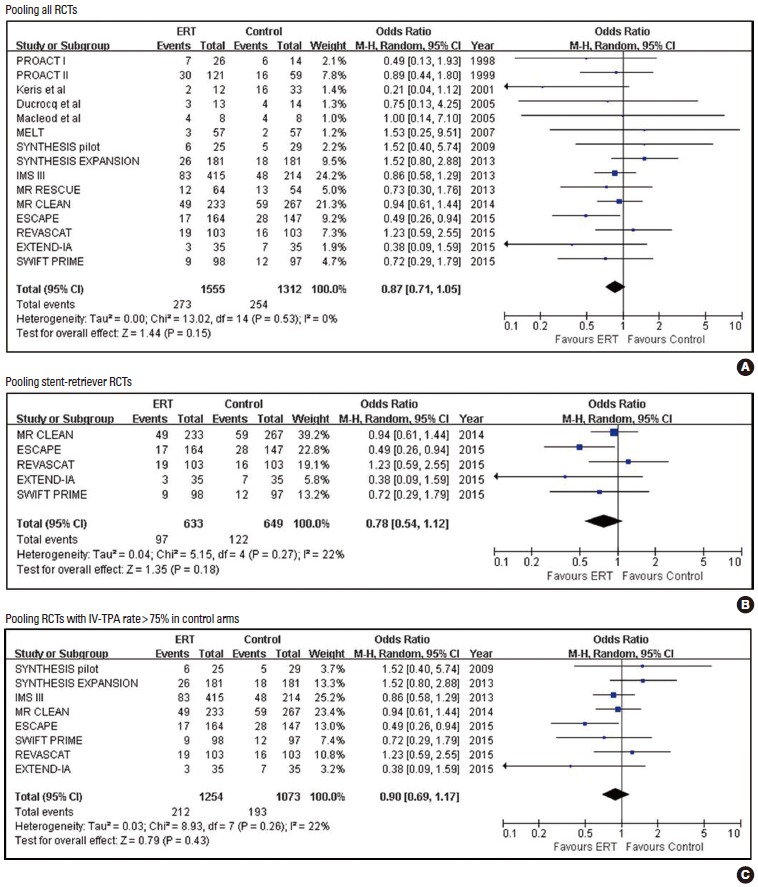
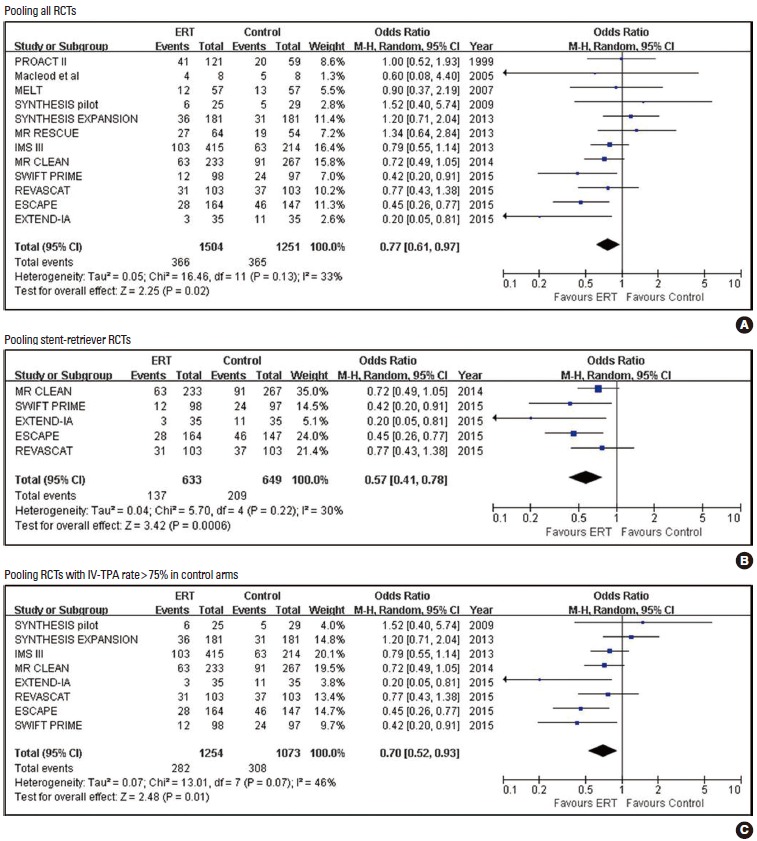
Results: We identified 15 relevant RCTs including 2,899 patients. For all trials, ERT was associated with increased good outcomes (odds ratio [OR] 1.79; 95% confidence interval [CI] 1.34, 2.40; P<0.001) compared to the control. ERT also increased no or minimal disability outcomes, good neurological recovery, good activity of daily living, and recanalization. ERT did not significantly increase symptomatic intracranial hemorrhage (SICH) (OR 1.19; 95% CI 0.83, 1.69; P=0.345) or death (OR 0.87; 95% CI 0.71, 1.05; P=0.151). In contrast, ERT significantly reduced extreme disability or death (OR 0.77; 95% CI 0.61, 0.97; P=0.025). Restricting to five stent-retriever trials comparing ERT plus IV-TPA vs. IV-TPA alone, the benefit was even greater for good outcome (OR 2.39; 95% CI 1.88, 3.04; P<0.001) and extreme disability or death (OR 0.57; 95% CI 0.41, 0.78; P=0.001). Restricting to eight RCTs comparing ERT (plus IV-TPA in six trials) with IV-TPA alone showed similar efficacy and safety.
Conclusions: This updated meta-analysis shows that ERT substantially improves clinical outcomes and reduces extreme disability or death without significantly increasing SICH compared to standard therapy.
Keywords: Acute ischemic stroke; Intra-arterial; Meta-analysis; Thrombectomy; Thrombolysis.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Tissue plasminogen activator for acute ischemic stroke The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Riedel CH, Zimmermann P, Jensen-Kondering U, Stingele R, Deuschl G, Jansen O. The importance of size: successful recanalization by intravenous thrombolysis in acute anterior stroke depends on thrombus length. Stroke. 2011;42:1775–1777. - PubMed
-
- Lee M, Hong KS, Saver JL. Efficacy of intra-arterial fibrinolysis for acute ischemic stroke: meta-analysis of randomized controlled trials. Stroke. 2010;41:932–937. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
