

Statins in Acute Ischemic Stroke: A Systematic Review
- PMID: 26437994
- PMCID: PMC4635713
- DOI: 10.5853/jos.2015.17.3.282
Statins in Acute Ischemic Stroke: A Systematic Review
Abstract
Background and purpose: Statins have pleiotropic effects of potential neuroprotection. However, because of lack of large randomized clinical trials, current guidelines do not provide specific recommendations on statin initiation in acute ischemic stroke (AIS). The current study aims to systematically review the statin effect in AIS.
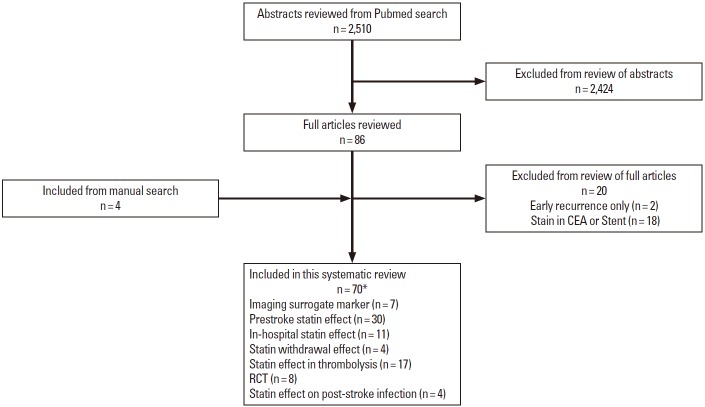
Methods: From literature review, we identified articles exploring prestroke and immediate post-stroke statin effect on imaging surrogate markers, initial stroke severity, functional outcome, and short-term mortality in human AIS. We summarized descriptive overview. In addition, for subjects with available data from publications, we conducted meta-analysis to provide pooled estimates.
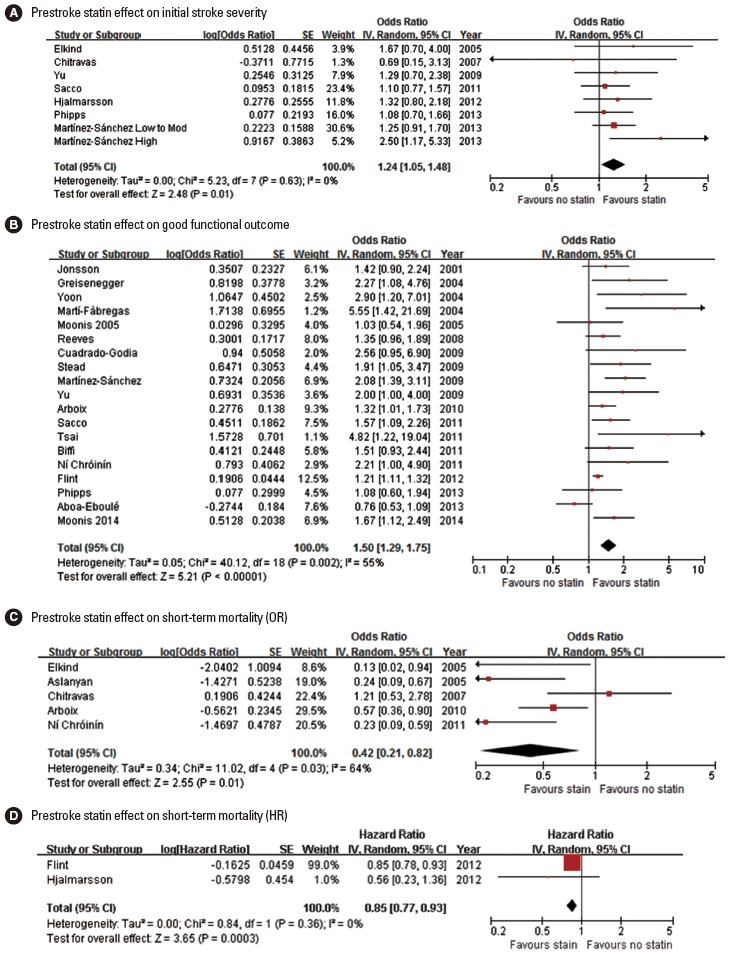
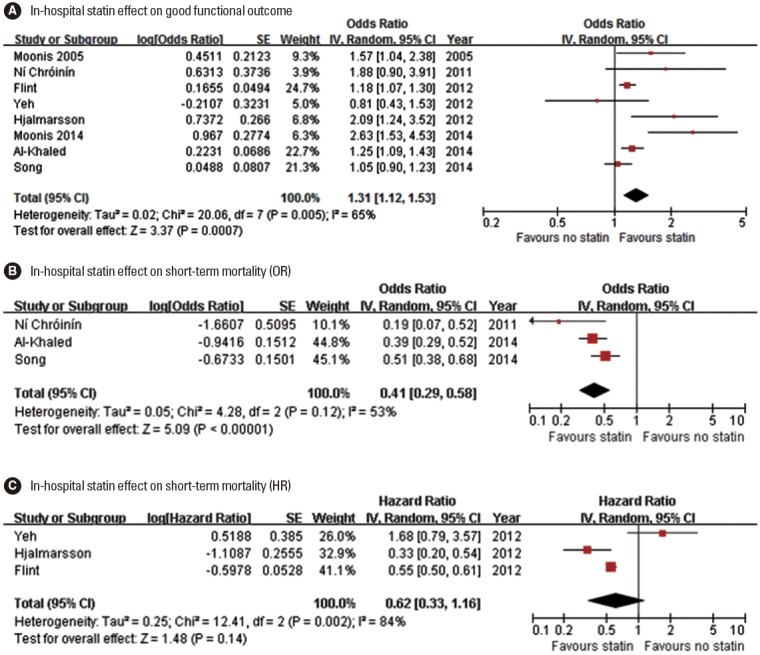
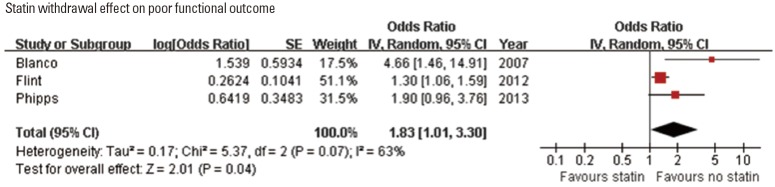
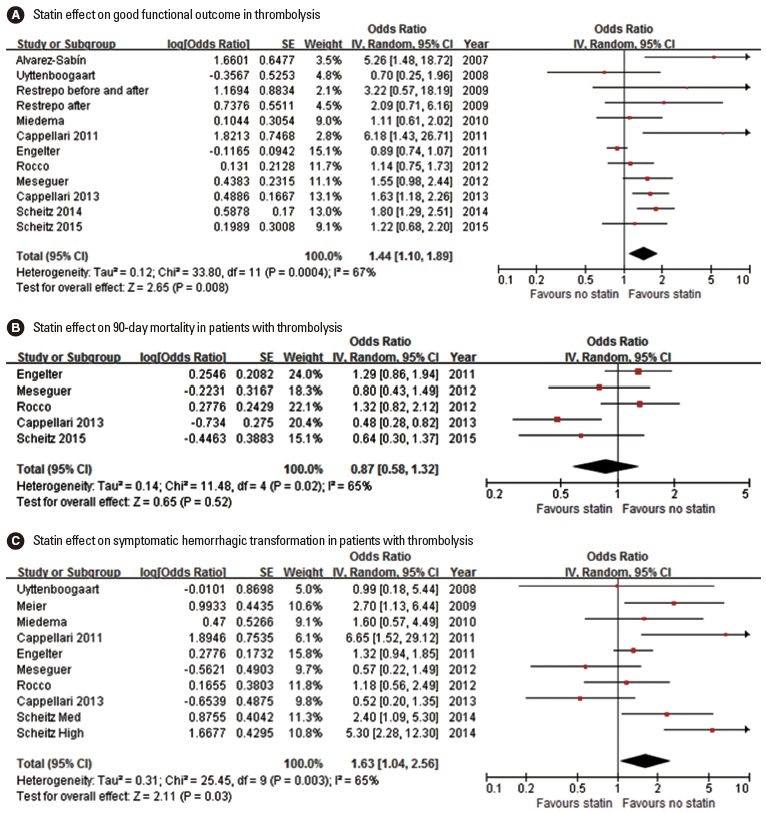
Results: In total, we identified 70 relevant articles including 6 meta-analyses. Surrogate imaging marker studies suggested that statin might enhance collaterals and reperfusion. Our updated meta-analysis indicated that prestroke statin use was associated with milder initial stroke severity (odds ratio [OR] [95% confidence interval], 1.24 [1.05-1.48]; P=0.013), good functional outcome (1.50 [1.29-1.75]; P<0.001), and lower mortality (0.42 [0.21-0.82]; P=0.0108). In-hospital statin use was associated with good functional outcome (1.31 [1.12-1.53]; P=0.001), and lower mortality (0.41 [0.29-0.58]; P<0.001). In contrast, statin withdrawal was associated with poor functional outcome (1.83 [1.01-3.30]; P=0.045). In patients treated with thrombolysis, statin was associated with good functional outcome (1.44 [1.10-1.89]; P=0.001), despite an increased risk of symptomatic hemorrhagic transformation (1.63 [1.04-2.56]; P=0.035).
Conclusions: The current study findings support the use of statin in AIS. However, the findings were mostly driven by observational studies at risk of bias, and thereby large randomized clinical trials would provide confirmatory evidence.
Keywords: Acute ischemic stroke; Mortality; Outcome; Statins; Stroke severity; Symptomatic hemorrhagic transformation.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Laufs U, Gertz K, Huang P, Nickenig G, Böhm M, Dirnagl U, et al. Atorvastatin upregulates type III nitric oxide synthase in thrombocytes, decreases platelet activation, and protects from cerebral ischemia in normocholesterolemic mice. Stroke. 2000;31:2442–2449. - PubMed
-
- Amin-Hanjani S, Stagliano NE, Yamada M, Huang PL, Liao JK, Moskowitz MA. Mevastatin, an HMG-CoA reductase inhibitor, reduces stroke damage and upregulates endothelial nitric oxide synthase in mice. Stroke. 2001;32:980–986. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
