

Extended Survival and Prognostic Factors for Patients With ALK-Rearranged Non-Small-Cell Lung Cancer and Brain Metastasis
- PMID: 26438117
- PMCID: PMC5070549
- DOI: 10.1200/JCO.2015.62.0138
Extended Survival and Prognostic Factors for Patients With ALK-Rearranged Non-Small-Cell Lung Cancer and Brain Metastasis
Abstract
Purpose: We performed a multi-institutional study to identify prognostic factors and determine outcomes for patients with ALK-rearranged non-small-cell lung cancer (NSCLC) and brain metastasis.
Patients and methods: A total of 90 patients with brain metastases from ALK-rearranged NSCLC were identified from six institutions; 84 of 90 patients received radiotherapy to the brain (stereotactic radiosurgery [SRS] or whole-brain radiotherapy [WBRT]), and 86 of 90 received tyrosine kinase inhibitor (TKI) therapy. Estimates for overall (OS) and intracranial progression-free survival were determined and clinical prognostic factors were identified by Cox proportional hazards modeling.
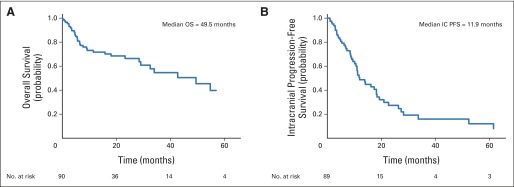
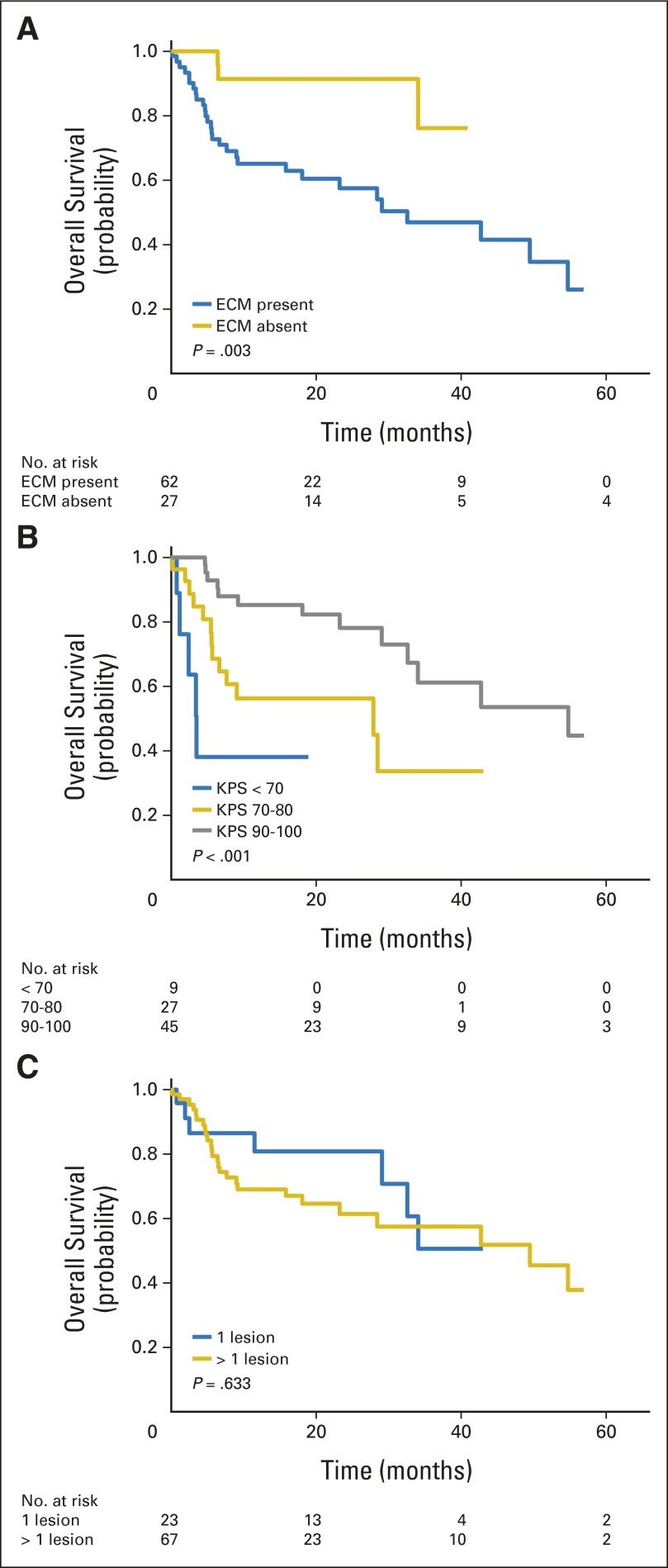
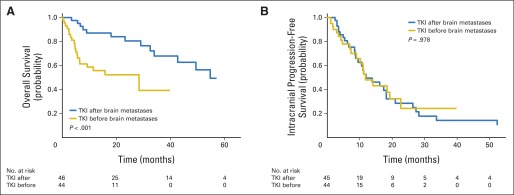
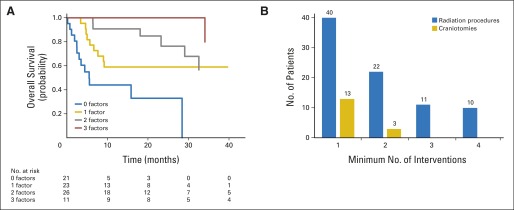
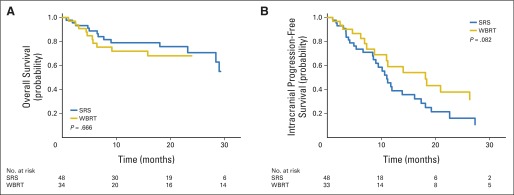
Results: Median OS after development of brain metastases was 49.5 months (95% CI, 29.0 months to not reached), and median intracranial progression-free survival was 11.9 months (95% CI, 10.1 to 18.2 months). Forty-five percent of patients with follow-up had progressive brain metastases at death, and repeated interventions for brain metastases were common. Absence of extracranial metastases, Karnofsky performance score ≥ 90, and no history of TKIs before development of brain metastases were associated with improved survival (P = .003, < .001, and < .001, respectively), whereas a single brain metastasis or initial treatment with SRS versus WBRT were not (P = .633 and .666, respectively). Prognostic factors significant by multivariable analysis were used to describe four patient groups with 2-year OS estimates of 33%, 59%, 76%, and 100%, respectively (P < .001).
Conclusion: Patients with brain metastases from ALK-rearranged NSCLC treated with radiotherapy (SRS and/or WBRT) and TKIs have prolonged survival, suggesting that interventions to control intracranial disease are critical. The refinement of prognosis for this molecular subtype of NSCLC identifies a population of patients likely to benefit from first-line SRS, close CNS observation, and treatment of emergent CNS disease.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Comment in
-
CNS Metastases in Patients With Non-Small-Cell Lung Cancer and ALK Gene Rearrangement.J Clin Oncol. 2016 Jan 10;34(2):107-9. doi: 10.1200/JCO.2015.63.9682. Epub 2015 Nov 30. J Clin Oncol. 2016. PMID: 26628475 No abstract available.
-
Is It Time to Reconsider Prophylactic Cranial Radiation in Non-Small-Cell Lung Cancer?J Clin Oncol. 2016 Jul 1;34(19):2314. doi: 10.1200/JCO.2015.65.2974. Epub 2016 Apr 25. J Clin Oncol. 2016. PMID: 27114597 No abstract available.
-
Reply to M.S. Copur et al and to M.C. Chamberlain.J Clin Oncol. 2016 Jul 1;34(19):2316-7. doi: 10.1200/JCO.2016.67.2816. Epub 2016 Apr 25. J Clin Oncol. 2016. PMID: 27114599 No abstract available.
-
Targetable Lung Cancer Brain Metastases: Improved Outcome.J Clin Oncol. 2016 Jul 1;34(19):2315. doi: 10.1200/JCO.2016.66.9465. Epub 2016 Apr 25. J Clin Oncol. 2016. PMID: 27114601 No abstract available.
References
-
- Sørensen JB, Hansen HH, Hansen M, et al. Brain metastases in adenocarcinoma of the lung: Frequency, risk groups, and prognosis. J Clin Oncol. 1988;6:1474–1480. - PubMed
-
- Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. 1997;37:745–751. - PubMed
-
- Gaspar LE, Scott C, Murray K, et al. Validation of the RTOG recursive partitioning analysis (RPA) classification for brain metastases. Int J Radiat Oncol Biol Phys. 2000;47:1001–1006. - PubMed
-
- Sperduto PW, Berkey B, Gaspar LE, et al. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1,960 patients in the RTOG database. Int J Radiat Oncol Biol Phys. 2008;70:510–514. - PubMed
-
- Sperduto CM, Watanabe Y, Mullan J, et al. A validation study of a new prognostic index for patients with brain metastases: The graded prognostic assessment. J Neurosurg. 2008;109(suppl):87–89. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
