

Sample selection, recruitment and participation rates in health examination surveys in Europe--experience from seven national surveys
- PMID: 26438235
- PMCID: PMC4595185
- DOI: 10.1186/s12874-015-0072-4
Sample selection, recruitment and participation rates in health examination surveys in Europe--experience from seven national surveys
Abstract
Background: Health examination surveys (HESs), carried out in Europe since the 1950's, provide valuable information about the general population's health for health monitoring, policy making, and research. Survey participation rates, important for representativeness, have been falling. International comparisons are hampered by differing exclusion criteria and definitions for non-response.
Method: Information was collected about seven national HESs in Europe conducted in 2007-2012. These surveys can be classified into household and individual-based surveys, depending on the sampling frames used. Participation rates of randomly selected adult samples were calculated for four survey modules using standardised definitions and compared by sex, age-group, geographical areas within countries, and over time, where possible.
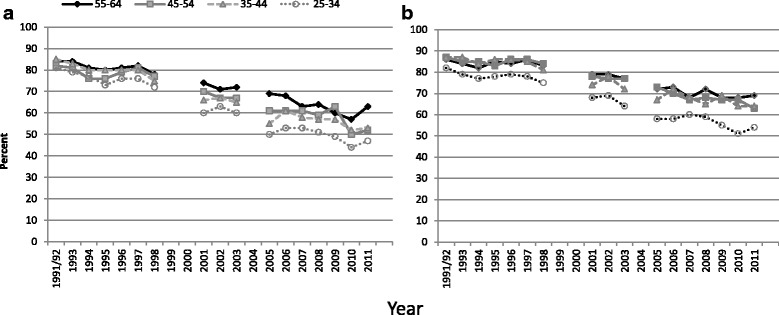
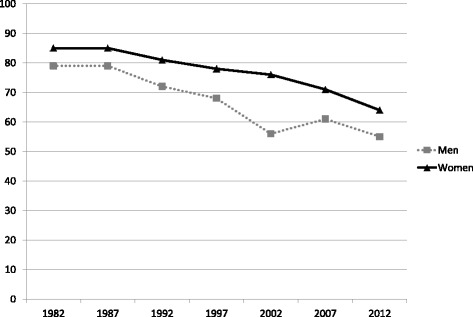
Results: All surveys covered residents not just citizens; three countries excluded those in institutions. In two surveys, physical examinations and blood sample collection were conducted at the participants' home; the others occurred at examination clinics. Recruitment processes varied considerably between surveys. Monetary incentives were used in four surveys. Initial participation rates aged 35-64 were 45% in the Netherlands (phase II), 54% in Germany (new and previous participants combined), 55% in Italy, and 65% in Finland. In Ireland, England and Scotland, household participation rates were 66%, 66% and 63% respectively. Participation rates were generally higher in women and increased with age. Almost all participants attending an examination centre agreed to all modules but surveys conducted in the participants' home had falling responses to each stage. Participation rates in most primate cities were substantially lower than the national average. Age-standardized response rates to blood pressure measurement among those aged 35-64 in Finland, Germany and England fell by 0.7-1.5 percentage points p.a. between 1998-2002 and 2010-2012. Longer trends in some countries show a more marked fall.
Conclusions: The coverage of the general population in these seven national HESs was good, based on the sampling frames used and the sample sizes. Pre-notification and reminders were used effectively in those with highest participation rates. Participation rates varied by age, sex, geographical area, and survey design. They have fallen in most countries; the Netherlands data shows that they can be maintained at higher levels but at much higher cost.
Figures


References
-
- Grotvedt L, Kuulasmaa K, Tolonen H, Heldal J, Graff-Iversen S, et al. 7. Sampling and recruitment. In: Tolonen H, Koponen P, Aromaa A, Conti S, Graff-Iversen S, Grotvedt L, Kanieff M, Mindell J, Natunen S, Primatesta P, et al., editors. Review of Health Examination Surveys in Europe. Helsinki: Publications of the National Public Health Institute B18/2008; 2008.
-
- STEPwise approach to surveillance (STEPS) http://www.who.int/chp/steps/en/ (Accessed 07/09/2015)
-
- Borodulin K, Vartiainen E, Peltonen M, et al. Fourty-year trends in cardiovascular risk factors in Finland. Eur J Public Health. 2014. - PubMed
-
- Tolonen H, Koponen P, Mindell JS, Mannisto S, Giampaoli S, Dias CM, et al. Under-estimation of obesity, hypertension and high cholesterol by self-reported data: Comparison of self-reported information and objective measures from health examination surveys. Eur J Public Health. 2014, doi:10.1093/eurpub/cku074. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
