

Social inequalities in a population based colorectal cancer screening programme in the Basque Country
- PMID: 26438240
- PMCID: PMC4594998
- DOI: 10.1186/s12889-015-2370-5
Social inequalities in a population based colorectal cancer screening programme in the Basque Country
Abstract
Background: While it is known that a variety of factors (biological, behavioural and interventional) play a major role in the health of individuals and populations, the importance of the role of social determinants is less clear. The effect of social inequality on population-based screening for colorectal cancer (CRC) could limit the value of such programmes. The present study aims to determine whether such inequalities exist.
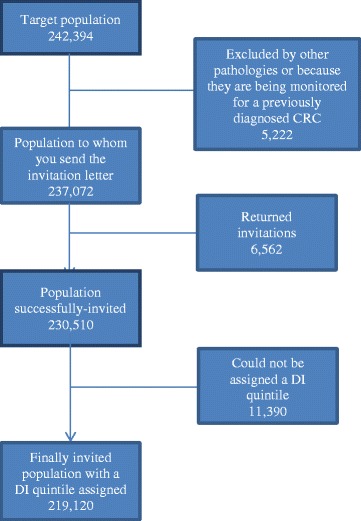
Methods: Data was obtained from the population-based screening programme administered in the Autonomous Community of the Basque Country, Spain, with a target population aged 50 to 69, first invited to participate between 2009 and 2011. The magnitude of inequality was analysed using the odds ratio (taking the least disadvantaged socioeconomic quintile as the reference population), the population attributable risk and the relative index of inequality, based on the regression, which is the ratio of the rates in the most and least disadvantaged socioeconomic groups.
Results: The target population comprised 242,394 people, with the test kit successfully sent to 95.1 % (230,510). The overall response rate was 64.3 % (67.1 in women and 61.4 % men). Among women, the highest participation was in the third quintile (71.5 %) and the lowest in the first - the least disadvantaged (65.7 %). The lowest and highest rates of people with identified lesions were in the second and fourth quintiles (14.7/1000 and 17.0/1000 respectively). Among men, the response rate was lowest in the fifth - most disadvantaged - quintile (60.2 %). The highest rate of identified lesions was in the fifth quintile; 38 % higher than the first (55.7/1000 compared to 41.0/1000).
Conclusions: Sex and socioeconomic group influence the rate of participation in the CRC programme and the rate of lesions found in the participants. Any public health programme is morally and ethically obliged to strive for equity and effectiveness. Improving participation of men and socially disadvantaged groups should be taken in account.
References
-
- CSDH . Closing the gap in a generation: health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health. Geneva: World Health Organization; 2008. - PubMed
-
- Marmot M, Wilkinson RG. Social determinants of health. 2. Oxford: Oxford University Press; 2006.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
