

Hospital Use in the Last Year of Life for Children With Life-Threatening Complex Chronic Conditions
- PMID: 26438707
- PMCID: PMC4621793
- DOI: 10.1542/peds.2015-0260
Hospital Use in the Last Year of Life for Children With Life-Threatening Complex Chronic Conditions
Abstract
Background and objectives: Although many adults experience resource-intensive and costly health care in the last year of life, less is known about these health care experiences in children with life-threatening complex chronic conditions (LT-CCCs). We assessed hospital resource use in children by type and number of LT-CCCs.
Methods: A retrospective analysis of 1252 children with LT-CCCs, ages 1 to 18 years, who died in 2012 within 40 US children's hospitals of the Pediatric Health Information System database. LT-CCCs were identified with International Classification of Diseases, 9th Revision, Clinical Modification codes. Using generalized linear models, we assessed hospital admissions, days, costs, and interventions (mechanical ventilation and surgeries) in the last year of life by type and number of LT-CCCs.
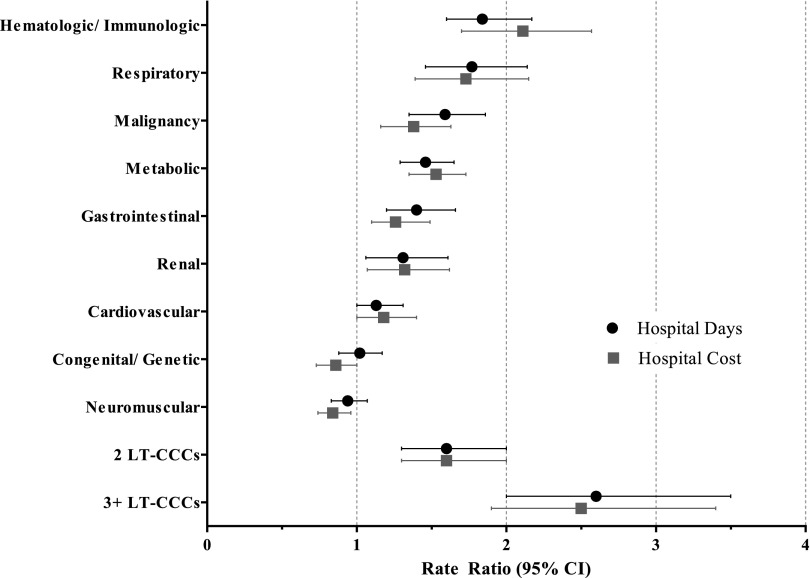
Results: In the last year of life, children with LT-CCCs experienced a median of 2 admissions (interquartile range [IQR] 1-5), 27 hospital days (IQR 7-84), and $142 562 (IQR $45 270-$410 087) in hospital costs. During the terminal admission, 76% (n = 946) were mechanically ventilated; 36% (n = 453) underwent surgery. Hospital use was greatest (P < .001) among children with hematologic/immunologic conditions (99 hospital days [IQR 51-146]; cost = $504 145 [IQR $250 147-$879 331]) and children with ≥3 LT-CCCs (75 hospital days [IQR 28-132]; cost = $341 222 [IQR $146 698-$686 585]).
Conclusions: Hospital use for children with LT-CCCs in the last year of life varies significantly across the type and number of conditions. Children with hematologic/immunologic or multiple conditions have the greatest hospital use. This information may be useful for clinicians striving to improve care for children with LT-CCCs nearing the end of life.
Copyright © 2015 by the American Academy of Pediatrics.
Figures
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-Of-Life Peer Group . Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32(3):638–643 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
