

Effect of Laparoscopic-Assisted Resection vs Open Resection of Stage II or III Rectal Cancer on Pathologic Outcomes: The ACOSOG Z6051 Randomized Clinical Trial
- PMID: 26441179
- PMCID: PMC5140087
- DOI: 10.1001/jama.2015.10529
Effect of Laparoscopic-Assisted Resection vs Open Resection of Stage II or III Rectal Cancer on Pathologic Outcomes: The ACOSOG Z6051 Randomized Clinical Trial
Abstract
Importance: Evidence about the efficacy of laparoscopic resection of rectal cancer is incomplete, particularly for patients with more advanced-stage disease.
Objective: To determine whether laparoscopic resection is noninferior to open resection, as determined by gross pathologic and histologic evaluation of the resected proctectomy specimen.
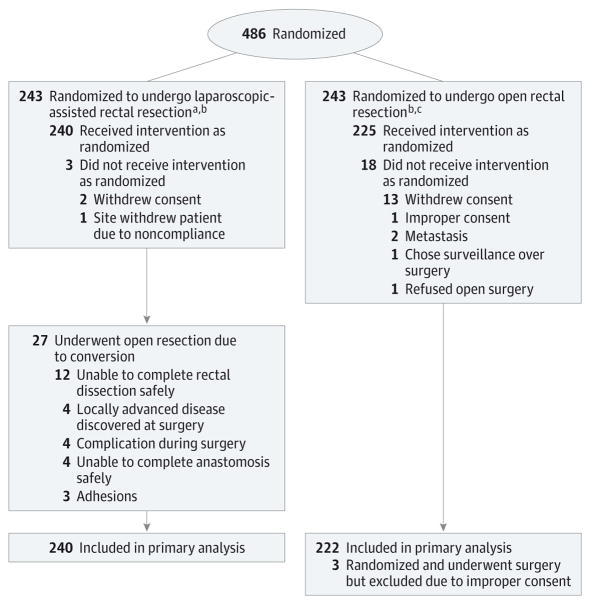
Design, setting, and participants: A multicenter, balanced, noninferiority, randomized trial enrolled patients between October 2008 and September 2013. The trial was conducted by credentialed surgeons from 35 institutions in the United States and Canada. A total of 486 patients with clinical stage II or III rectal cancer within 12 cm of the anal verge were randomized after completion of neoadjuvant therapy to laparoscopic or open resection.
Interventions: Standard laparoscopic and open approaches were performed by the credentialed surgeons.
Main outcomes and measures: The primary outcome assessing efficacy was a composite of circumferential radial margin greater than 1 mm, distal margin without tumor, and completeness of total mesorectal excision. A 6% noninferiority margin was chosen according to clinical relevance estimation.
Results: Two hundred forty patients with laparoscopic resection and 222 with open resection were evaluable for analysis of the 486 enrolled. Successful resection occurred in 81.7% of laparoscopic resection cases (95% CI, 76.8%-86.6%) and 86.9% of open resection cases (95% CI, 82.5%-91.4%) and did not support noninferiority (difference, -5.3%; 1-sided 95% CI, -10.8% to ∞; P for noninferiority = .41). Patients underwent low anterior resection (76.7%) or abdominoperineal resection (23.3%). Conversion to open resection occurred in 11.3% of patients. Operative time was significantly longer for laparoscopic resection (mean, 266.2 vs 220.6 minutes; mean difference, 45.5 minutes; 95% CI, 27.7-63.4; P < .001). Length of stay (7.3 vs 7.0 days; mean difference, 0.3 days; 95% CI, -0.6 to 1.1), readmission within 30 days (3.3% vs 4.1%; difference, -0.7%; 95% CI, -4.2% to 2.7%), and severe complications (22.5% vs 22.1%; difference, 0.4%; 95% CI, -4.2% to 2.7%) did not differ significantly. Quality of the total mesorectal excision specimen in 462 operated and analyzed surgeries was complete (77%) and nearly complete (16.5%) in 93.5% of the cases. Negative circumferential radial margin was observed in 90% of the overall group (87.9% laparoscopic resection and 92.3% open resection; P = .11). Distal margin result was negative in more than 98% of patients irrespective of type of surgery (P = .91).
Conclusions and relevance: Among patients with stage II or III rectal cancer, the use of laparoscopic resection compared with open resection failed to meet the criterion for noninferiority for pathologic outcomes. Pending clinical oncologic outcomes, the findings do not support the use of laparoscopic resection in these patients.
Trial registration: clinicaltrials.gov Identifier: NCT00726622.
Figures
Comment in
-
Minimally Invasive Approaches to Rectal Cancer and Diverticulitis: Does Less Mean More?JAMA. 2015 Oct 6;314(13):1343-5. doi: 10.1001/jama.2015.11454. JAMA. 2015. PMID: 26441178 No abstract available.
-
Laparoscopic rectal cancer resection: inferior to open or not?Colorectal Dis. 2016 Mar;18(3):233. doi: 10.1111/codi.13270. Colorectal Dis. 2016. PMID: 26934849 No abstract available.
-
Outcomes of Open vs Laparoscopic Rectal Cancer Resection.JAMA Oncol. 2017 Jan 1;3(1):115-116. doi: 10.1001/jamaoncol.2016.3205. JAMA Oncol. 2017. PMID: 27684053 No abstract available.
-
What quality criterion should we choose to evaluate the surgical resection of rectal cancer?J Visc Surg. 2017 Apr;154(2):69-71. doi: 10.1016/j.jviscsurg.2016.12.001. Epub 2017 Jan 30. J Visc Surg. 2017. PMID: 28153519 No abstract available.
-
Oncologic results of conventional laparoscopic TME: is the intramesorectal plane really acceptable?Tech Coloproctol. 2018 Nov;22(11):831-834. doi: 10.1007/s10151-018-1901-3. Epub 2018 Dec 17. Tech Coloproctol. 2018. PMID: 30560320 No abstract available.
References
-
- Dorrance HR, Docherty GM, O’Dwyer PJ. Effect of surgeon specialty interest on patient outcome after potentially curative colorectal cancer surgery. Dis Colon Rectum. 2000;43(4):492–498. - PubMed
-
- Monson JR, Weiser MR, Buie WD, et al. Standards Practice Task Force of the American Society of Colon and Rectal Surgeons. Practice parameters for the management of rectal cancer (revised) Dis Colon Rectum. 2013;56(5):535–550. - PubMed
-
- Quirke P, Steele R, Monson J, et al. MRC CR07/NCIC-CTG CO16 Trial Investigators; NCRI Colorectal Cancer Study Group. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet. 2009;373(9666):821–828. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
