

Health Coaching Reduces HbA1c in Type 2 Diabetic Patients From a Lower-Socioeconomic Status Community: A Randomized Controlled Trial
- PMID: 26441467
- PMCID: PMC4642794
- DOI: 10.2196/jmir.4871
Health Coaching Reduces HbA1c in Type 2 Diabetic Patients From a Lower-Socioeconomic Status Community: A Randomized Controlled Trial
Abstract
Background: Adoptions of health behaviors are crucial for maintaining good health after type 2 diabetes mellitus (T2DM) diagnoses. However, adherence to glucoregulating behaviors like regular exercise and balanced diet can be challenging, especially for people living in lower-socioeconomic status (SES) communities. Providing cost-effective interventions that improve self-management is important for improving quality of life and the sustainability of health care systems.
Objective: To evaluate a health coach intervention with and without the use of mobile phones to support health behavior change in patients with type 2 diabetes.
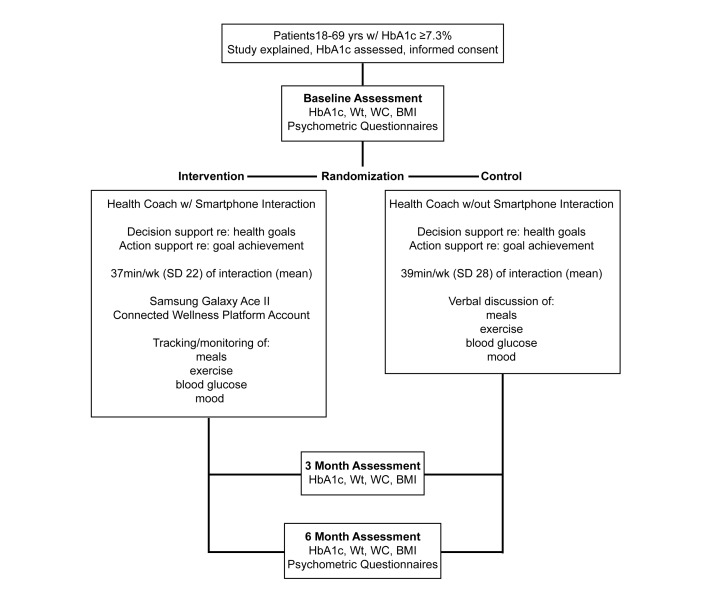
Methods: In this noninferiority, pragmatic randomized controlled trial (RCT), patients from two primary care health centers in Toronto, Canada, with type 2 diabetes and a glycated hemoglobin/hemoglobin A1c (HbA1c) level of ≥7.3% (56.3 mmol/mol) were randomized to receive 6 months of health coaching with or without mobile phone monitoring support. We hypothesized that both approaches would result in significant HbA1c reductions, although health coaching with mobile phone monitoring would result in significantly larger effects. Participants were evaluated at baseline, 3 months, and 6 months. The primary outcome was the change in HbA1c from baseline to 6 months (difference between and within groups). Other outcomes included weight, waist circumference, body mass index (BMI), satisfaction with life, depression and anxiety (Hospital Anxiety and Depression Scale [HADS]), positive and negative affect (Positive and Negative Affect Schedule [PANAS]), and quality of life (Short Form Health Survey-12 [SF-12]).
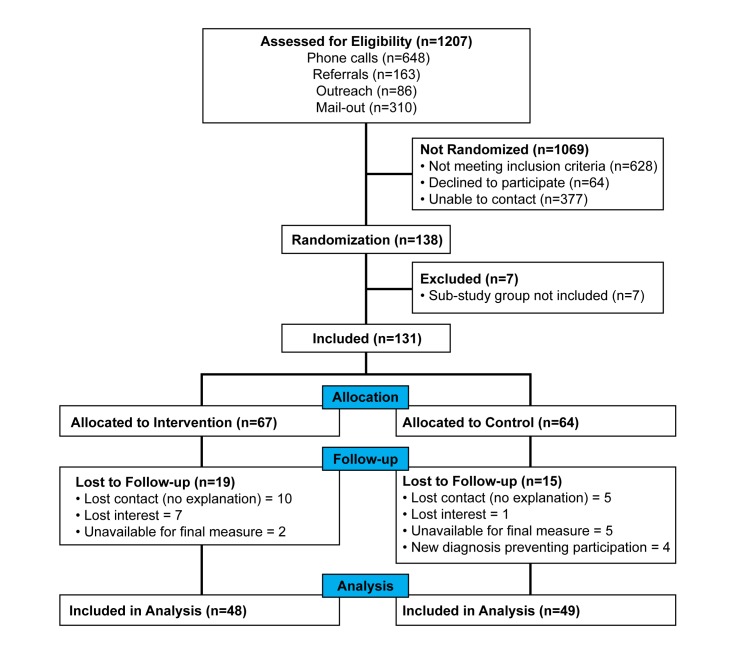
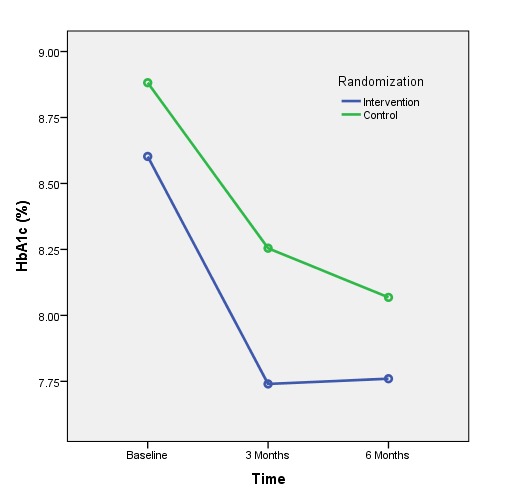
Results: A total of 138 patients were randomized and 7 were excluded for a substudy; of the remaining 131, 67 were allocated to the intervention group and 64 to the control group. Primary outcome data were available for 97 participants (74.0%). While both groups reduced their HbA1c levels, there were no significant between-group differences in change of HbA1c at 6 months using intention-to-treat (last observation carried forward [LOCF]) (P=.48) or per-protocol (P=.83) principles. However, the intervention group did achieve an accelerated HbA1c reduction, leading to a significant between-group difference at 3 months (P=.03). This difference was reduced at the 6-month follow-up as the control group continued to improve, achieving a reduction of 0.81% (8.9 mmol/mol) (P=.001) compared with a reduction of 0.84% (9.2 mmol/mol)(P=.001) in the intervention group. Intervention group participants also had significant decreases in weight (P=.006) and waist circumference (P=.01) while controls did not. Both groups reported improvements in mood, satisfaction with life, and quality of life.
Conclusions: Health coaching with and without access to mobile technology appeared to improve glucoregulation and mental health in a lower-SES, T2DM population. The accelerated improvement in the mobile phone group suggests the connectivity provided may more quickly improve adoption and adherence to health behaviors within a clinical diabetes management program. Overall, health coaching in primary care appears to lead to significant benefits for patients from lower-SES communities with poorly controlled type 2 diabetes.
Trial registration: ClinicalTrials.gov NCT02036892; http://clinicaltrials.gov/ct2/show/NCT02036892 (Archived by WebCite at http://www.webcitation.org/6b3cJYJOD).
Keywords: RCT; diabetes mellitus, type 2; health coaching; mHealth; randomized controlled trial; telehealth.
Conflict of interest statement
Conflicts of Interest: None Declared.
Figures
Similar articles
-
Telemonitoring and Mobile Phone-Based Health Coaching Among Finnish Diabetic and Heart Disease Patients: Randomized Controlled Trial.J Med Internet Res. 2015 Jun 17;17(6):e153. doi: 10.2196/jmir.4059. J Med Internet Res. 2015. PMID: 26084979 Free PMC article. Clinical Trial.
-
A Mobile Lifestyle Management Program (GlycoLeap) for People With Type 2 Diabetes: Single-Arm Feasibility Study.JMIR Mhealth Uhealth. 2019 May 24;7(5):e12965. doi: 10.2196/12965. JMIR Mhealth Uhealth. 2019. PMID: 31127720 Free PMC article.
-
A Fully Automated Web-Based Program Improves Lifestyle Habits and HbA1c in Patients With Type 2 Diabetes and Abdominal Obesity: Randomized Trial of Patient E-Coaching Nutritional Support (The ANODE Study).J Med Internet Res. 2017 Nov 8;19(11):e360. doi: 10.2196/jmir.7947. J Med Internet Res. 2017. PMID: 29117929 Free PMC article. Clinical Trial.
-
Psychological interventions to improve self-management of type 1 and type 2 diabetes: a systematic review.Health Technol Assess. 2020 Jun;24(28):1-232. doi: 10.3310/hta24280. Health Technol Assess. 2020. PMID: 32568666 Free PMC article.
-
Clinical Improvements by Telemedicine Interventions Managing Type 1 and Type 2 Diabetes: Systematic Meta-review.J Med Internet Res. 2021 Feb 19;23(2):e23244. doi: 10.2196/23244. J Med Internet Res. 2021. PMID: 33605889 Free PMC article.
Cited by
-
Barriers and facilitators to healthy active living in South Asian families in Canada: a thematic analysis.BMJ Open. 2022 Nov 11;12(11):e060385. doi: 10.1136/bmjopen-2021-060385. BMJ Open. 2022. PMID: 36368751 Free PMC article.
-
Human Coaching Methodologies for Automatic Electronic Coaching (eCoaching) as Behavioral Interventions With Information and Communication Technology: Systematic Review.J Med Internet Res. 2021 Mar 24;23(3):e23533. doi: 10.2196/23533. J Med Internet Res. 2021. PMID: 33759793 Free PMC article.
-
An Initial Test of the Efficacy of a Digital Health Intervention for Bariatric Surgery Candidates.Obes Surg. 2022 Nov;32(11):3641-3649. doi: 10.1007/s11695-022-06258-8. Epub 2022 Sep 8. Obes Surg. 2022. PMID: 36074201 Free PMC article. Clinical Trial.
-
The Influence of Age, Sex, and Socioeconomic Status on Glycemic Control Among People With Type 1 and Type 2 Diabetes in Canada: Patient-Led Longitudinal Retrospective Cross-sectional Study With Multiple Time Points of Measurement.JMIR Diabetes. 2023 Apr 27;8:e35682. doi: 10.2196/35682. JMIR Diabetes. 2023. PMID: 37104030 Free PMC article.
-
Patterns of User Engagement With the Mobile App, Manage My Pain: Results of a Data Mining Investigation.JMIR Mhealth Uhealth. 2017 Jul 12;5(7):e96. doi: 10.2196/mhealth.7871. JMIR Mhealth Uhealth. 2017. PMID: 28701291 Free PMC article.
References
-
- Wayne N, Ritvo P. Smartphone-enabled health coach intervention for people with diabetes from a modest socioeconomic strata community: single-arm longitudinal feasibility study. J Med Internet Res. 2014;16(6):e149. doi: 10.2196/jmir.3180. http://www.jmir.org/2014/6/e149/ v16i6e149 - DOI - PMC - PubMed
-
- Moore JO, Marshall MA, Judge DC, Moss FH, Gilroy SJ, Crocker JB, Zusman RM. Technology-supported apprenticeship in the management of hypertension: a randomized controlled trial. J Clin Outcomes Manag. 2014 Mar;21(3):110–122. http://turner-white.com/pdf/jcom_mar14_hypertension.pdf
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
