

Immunotherapy of Metastatic Colorectal Cancer: Prevailing Challenges and New Perspectives
- PMID: 26441489
- PMCID: PMC4591512
- DOI: 10.1007/s11888-015-0269-2
Immunotherapy of Metastatic Colorectal Cancer: Prevailing Challenges and New Perspectives
Abstract
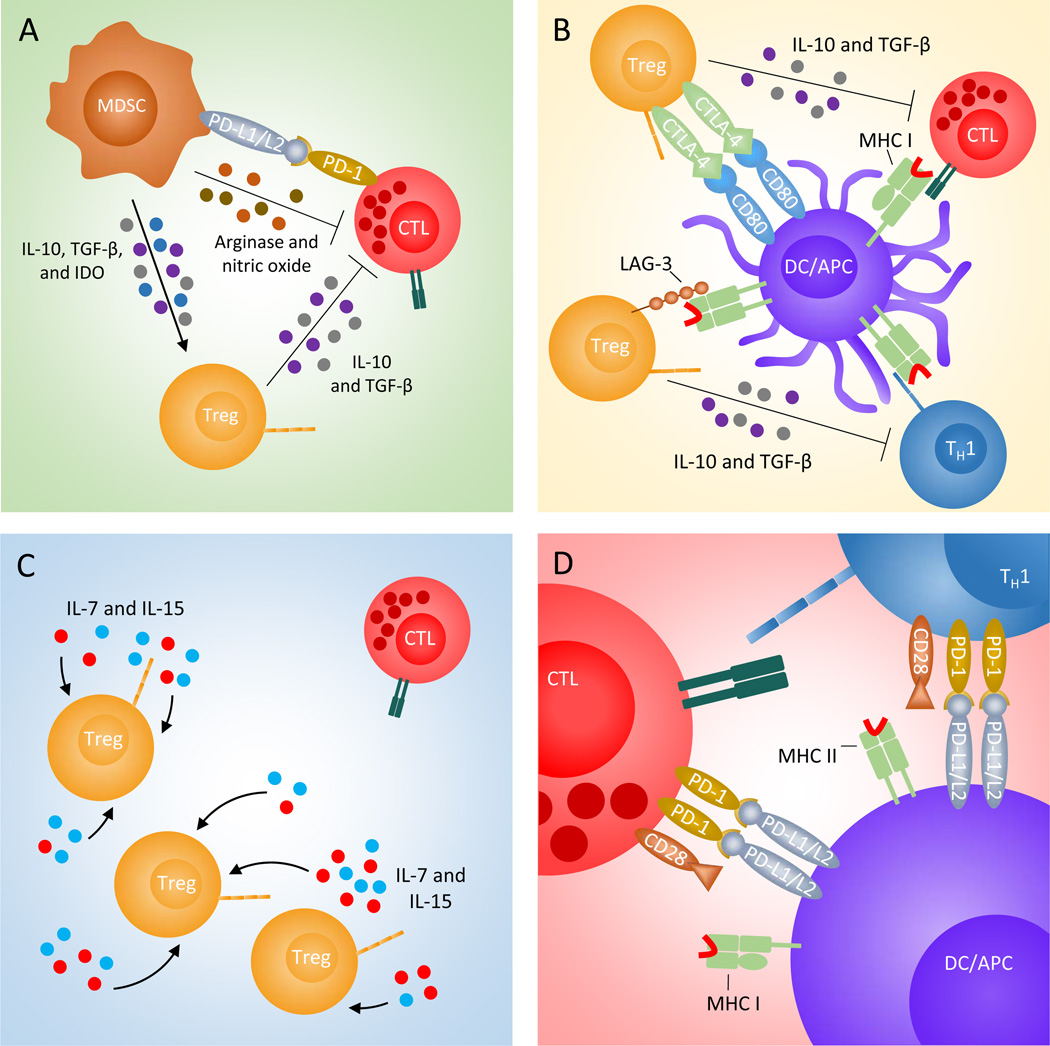
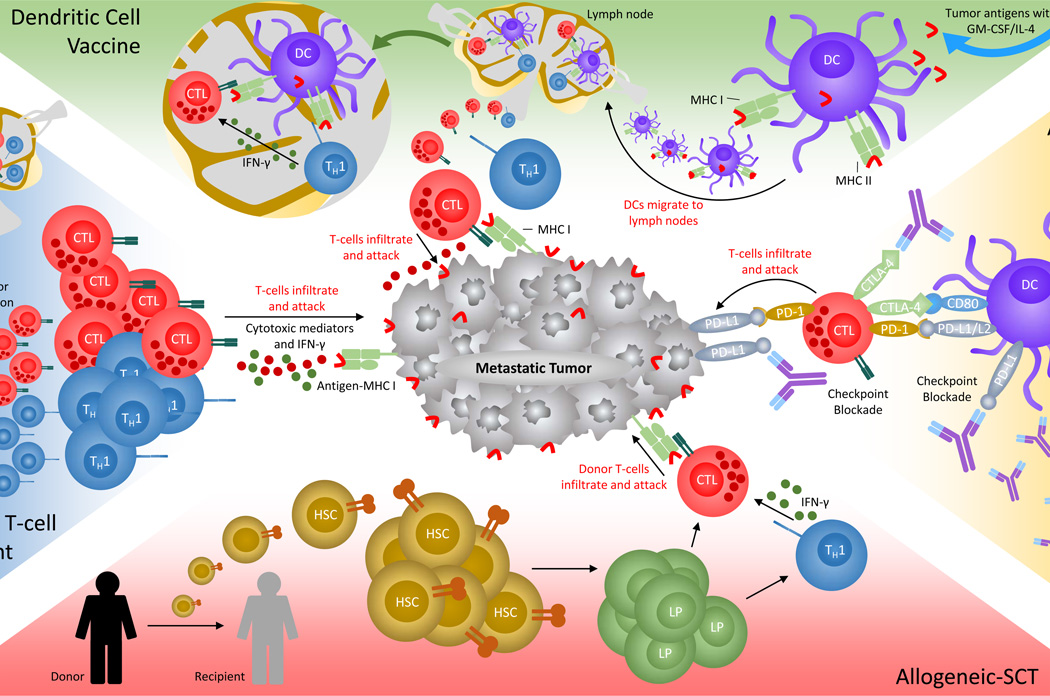
Patients with recurring or metastatic colorectal cancer (mCRC) have strikingly low long-term survival, while conventional treatments such as chemotherapeutic intervention and radiation therapy marginally improve longevity. Although, many factors involving immunosurveillance and immunosuppression were recently validated as important for patient prognosis and care, a multitude of experimental immunotherapies designed to combat unresectable mCRC have, in few cases, successfully mobilized antitumor immune cells against malignancies, nor conclusively or consistently granted protection, complete remission, and/or stable disease from immunotherapy - of which benefit less than 10% of those receiving therapy. After decades of progress, however, new insights into the mechanisms of immunosuppression, tolerance, and mutation profiling established novel therapies that circumvent these immunological barriers. This review underlines the most exciting methods to date that manipulate immune cells to curb mCRC, including adoptive cell therapy, dendritic cell vaccines, and checkpoint inhibitor antibodies - of which hint at effective and enduring protection against disease progression and undetected micrometastases.
Keywords: Adoptive Immunotherapy; Adoptive T-cell therapy; Allogeneic stem-cell transplant; Antibody therapy; Antitumor immunity; Biomarker; CTLA-4; Cytotoxic T-Lymphocyte; Dendritic cell; Helper T-Cell; Immunosuppression; Immunosurveillance; Immunotherapy; Ipilimumab; Macrophage; Metastatic colorectal cancer; Myeloid-derived suppressor cell; PD-1/L1; Regulatory T-cell; T-cell; Vaccine.
Figures
Similar articles
-
Clinically feasible approaches to potentiating cancer cell-based immunotherapies.Hum Vaccin Immunother. 2015;11(4):851-69. doi: 10.1080/21645515.2015.1009814. Hum Vaccin Immunother. 2015. PMID: 25933181 Free PMC article. Review.
-
The Next Immune-Checkpoint Inhibitors: PD-1/PD-L1 Blockade in Melanoma.Clin Ther. 2015 Apr 1;37(4):764-82. doi: 10.1016/j.clinthera.2015.02.018. Epub 2015 Mar 29. Clin Ther. 2015. PMID: 25823918 Free PMC article. Review.
-
Future perspectives in melanoma research : Meeting report from the "Melanoma Bridge". Napoli, December 1st-4th 2015.J Transl Med. 2016 Nov 15;14(1):313. doi: 10.1186/s12967-016-1070-y. J Transl Med. 2016. PMID: 27846884 Free PMC article.
-
Association of Survival and Immune-Related Biomarkers With Immunotherapy in Patients With Non-Small Cell Lung Cancer: A Meta-analysis and Individual Patient-Level Analysis.JAMA Netw Open. 2019 Jul 3;2(7):e196879. doi: 10.1001/jamanetworkopen.2019.6879. JAMA Netw Open. 2019. PMID: 31290993 Free PMC article.
-
The Evolving Role of Immune Checkpoint Inhibitors in Cancer Treatment.Oncologist. 2015 Jul;20(7):812-22. doi: 10.1634/theoncologist.2014-0422. Epub 2015 Jun 11. Oncologist. 2015. PMID: 26069281 Free PMC article. Review.
Cited by
-
Utility of Image Guidance in the Localization of Disappearing Colorectal Liver Metastases.J Gastrointest Surg. 2019 Apr;23(4):760-767. doi: 10.1007/s11605-019-04106-2. Epub 2019 Jan 24. J Gastrointest Surg. 2019. PMID: 30680630 Free PMC article.
-
Metastatic Colorectal Cancer Patient With Microsatellite Stability and BRAFV600E Mutation Showed a Complete Metabolic Response to PD-1 Blockade and Bevacizumab: A Case Report.Front Oncol. 2021 Apr 27;11:652394. doi: 10.3389/fonc.2021.652394. eCollection 2021. Front Oncol. 2021. PMID: 33987088 Free PMC article.
-
Therapeutic Approaches for Metastases from Colorectal Cancer and Pancreatic Ductal Carcinoma.Pharmaceutics. 2021 Jan 14;13(1):103. doi: 10.3390/pharmaceutics13010103. Pharmaceutics. 2021. PMID: 33466892 Free PMC article. Review.
-
Endothelial cells in colorectal cancer.World J Gastrointest Oncol. 2019 Nov 15;11(11):946-956. doi: 10.4251/wjgo.v11.i11.946. World J Gastrointest Oncol. 2019. PMID: 31798776 Free PMC article. Review.
-
Immunotherapy in Gastrointestinal Cancers.Biomed Res Int. 2017;2017:4346576. doi: 10.1155/2017/4346576. Epub 2017 Jul 3. Biomed Res Int. 2017. PMID: 28758114 Free PMC article. Review.
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015 Feb 4; - PubMed
-
- Cunningham D, Atkin W, Lenz HJ, Lynch HT, Minsky B, Nordlinger B, et al. Colorectal cancer. Lancet. 2010 Mar 20;375(9719):1030–1047. - PubMed
-
- Fong Y, Cohen AM, Fortner JG, Enker WE, Turnbull AD, Coit DG, et al. Liver resection for colorectal metastases. J Clin Oncol. 1997 Mar;15(3):938–946. - PubMed
-
- Van Cutsem E, Nordlinger B, Adam R, Kohne CH, Pozzo C, Poston G, et al. Towards a paneuropean consensus on the treatment of patients with colorectal liver metastases. Eur J Cancer. 2006 Sep;42(14):2212–2221. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
