

The Prevalence of Individual Histopathologic Features Varies according to Autoantibody Status in Muscle Biopsies from Patients with Dermatomyositis
- PMID: 26443871
- PMCID: PMC6544046
The Prevalence of Individual Histopathologic Features Varies according to Autoantibody Status in Muscle Biopsies from Patients with Dermatomyositis
Abstract
Objective: Individual dermatomyositis (DM)-associated autoantibodies are associated with distinct clinical phenotypes. This study was undertaken to explore the association of these autoantibodies with specific muscle biopsy features.
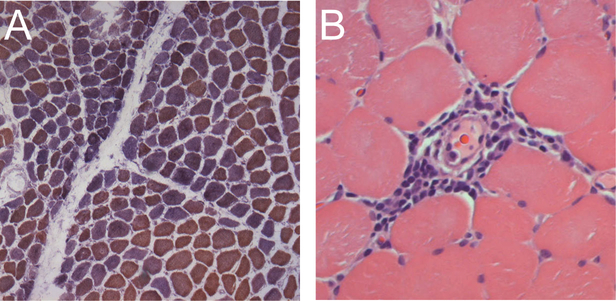
Methods: DM subjects with a muscle biopsy reviewed at Johns Hopkins had sera screened for autoantibodies recognizing Mi-2, transcriptional intermediary factor 1-γ (TIF1-γ), NXP2, MDA5, Ro52, PM-Scl, and Jo1. We also included anti-Jo1–positive patients with polymyositis (PM) who had a biopsy read at Johns Hopkins. Analyzed histological features included perifascicular atrophy, perivascular inflammation, mitochondrial dysfunction, primary inflammation, and myofiber necrosis. Duration of disease, biopsy location, and treatment at biopsy were also analyzed.
Results: We studied 91 DM and 7 anti-Jo1–positive patients with PM. In univariate analyses, TIF1-γ+ patients had more mitochondrial dysfunction (47% vs 18%; p = 0.05), NXP2+ patients had less primary inflammation (0% vs 28%; p = 0.01), Mi-2+ patients had more primary inflammation (50% vs 19%; p = 0.03), and PM-Scl+ patients had more primary inflammation (67% vs 18%; p = 0.004) than those who were negative for each autoantibody. Although reliability was limited because of small sample numbers, multivariate analysis confirmed that TIF1-γ+ patients had more mitochondrial dysfunction [prevalence ratio (PR) 2.6, 95% CI 1.0–6.5, p = 0.05] and PM-Scl+ patients had more primary inflammation (PR 5.2, 95% CI 2.0–13.4; p = 0.001) independent of disease duration at biopsy, biopsy site, and treatment at biopsy. No differences in muscle biopsy features were noted between anti-Jo1–positive patients diagnosed with DM and PM.
Conclusion: The prevalence of different histological features varies according to autoantibody status in DM. Muscle biopsy features are similar in anti-Jo1 patients with and without a rash.
Figures
References
-
- Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med 1975;292:403–7. - PubMed
-
- Hoogendijk JE, Amato AA, Lecky BR, Choy EH, Lundberg IE, Rose MR, et al. 119th ENMC international workshop: trial design in adult idiopathic inflammatory myopathies, with the exception of inclusion body myositis, 10–12 October 2003, Naarden, The Netherlands. Neuromuscul Disord 2004;14:337–45. - PubMed
-
- Dalakas MC, Hohlfeld R. Polymyositis and dermatomyositis. Lancet 2003;362:971–82. - PubMed
-
- Tanimoto K, Nakano K, Kano S, Mori S, Ueki H, Nishitani H, et al. Classification criteria for polymyositis and dermatomyositis. J Rheumatol 1995;22:668–74. - PubMed
-
- Targoff IN, Miller FW, Medsger TA Jr, Oddis CV. Classification criteria for the idiopathic inflammatory myopathies. Curr Opin Rheumatol 1997;9:527–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous