

Intraoperative Goal-directed Fluid Therapy in Elective Major Abdominal Surgery: A Meta-analysis of Randomized Controlled Trials
- PMID: 26445470
- PMCID: PMC4741406
- DOI: 10.1097/SLA.0000000000001366
Intraoperative Goal-directed Fluid Therapy in Elective Major Abdominal Surgery: A Meta-analysis of Randomized Controlled Trials
Abstract
Objectives: To compare the effects of intraoperative goal-directed fluid therapy (GDFT) with conventional fluid therapy, and determine whether there was a difference in outcome between studies that did and did not use Enhanced Recovery After Surgery (ERAS) protocols.
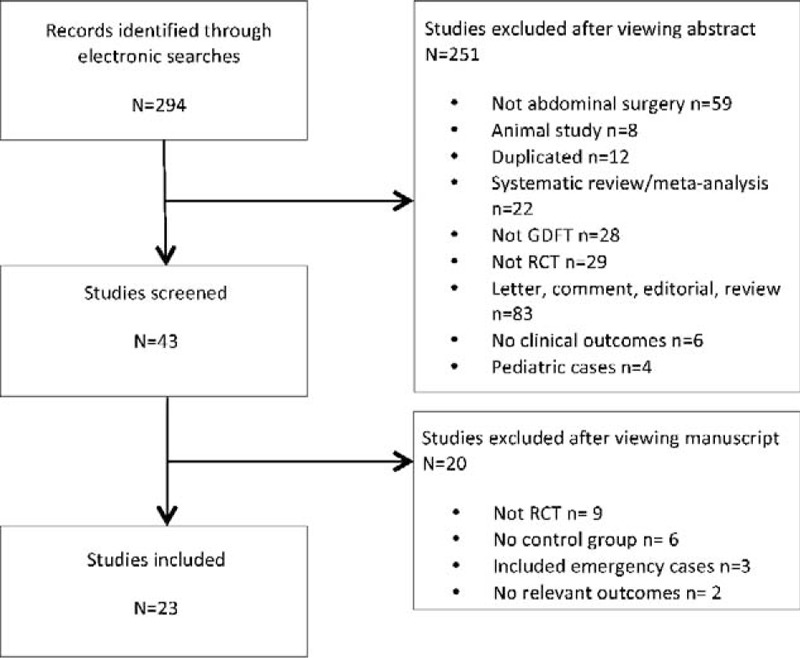
Methods: Meta-analysis of randomized controlled trials of adult patients undergoing elective major abdominal surgery comparing intraoperative GDFT versus conventional fluid therapy. The outcome measures were postoperative morbidity, length of stay, gastrointestinal function and 30-day mortality.
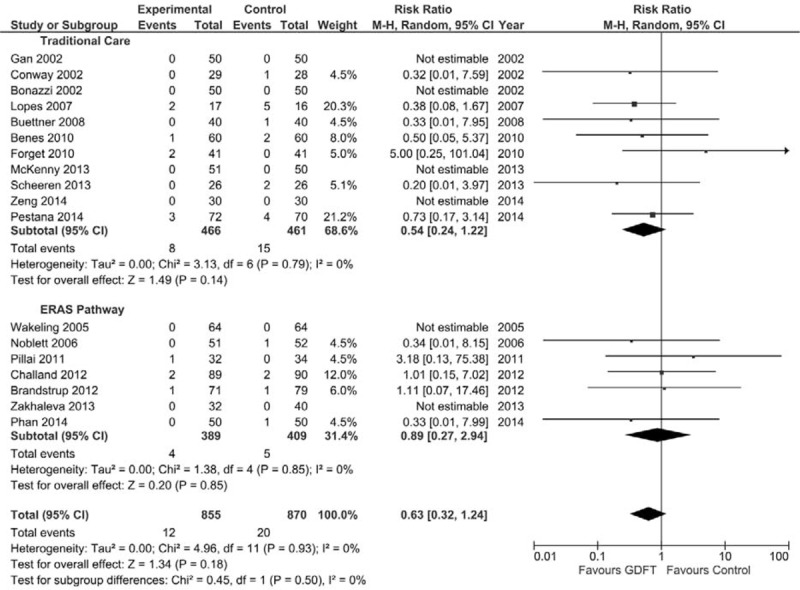
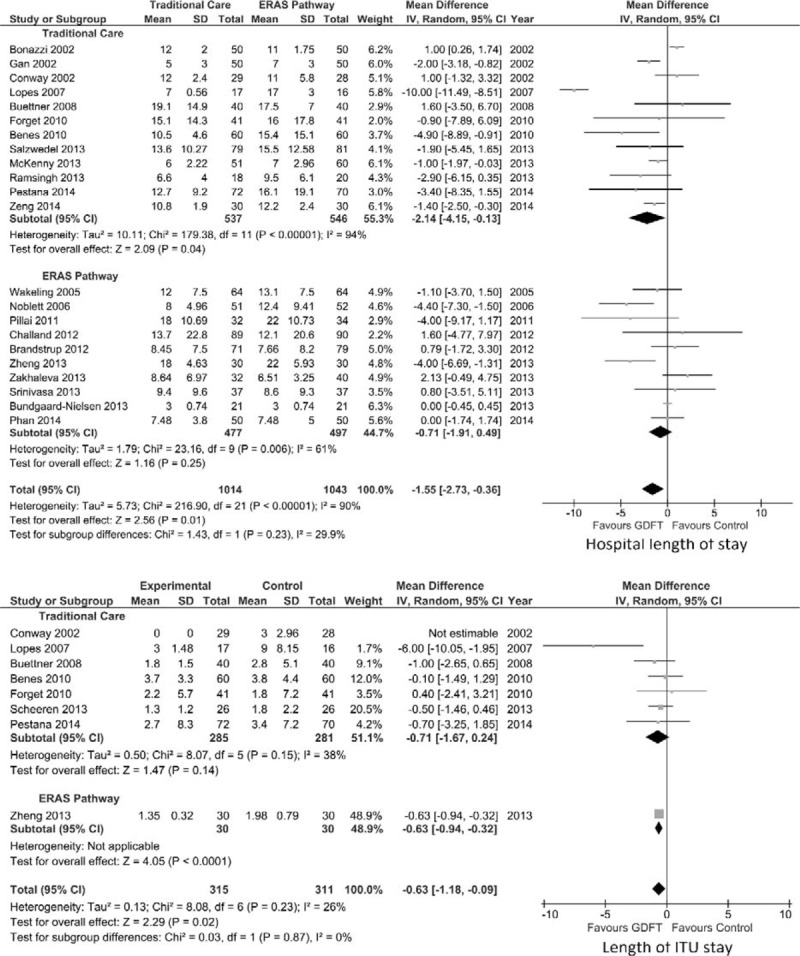
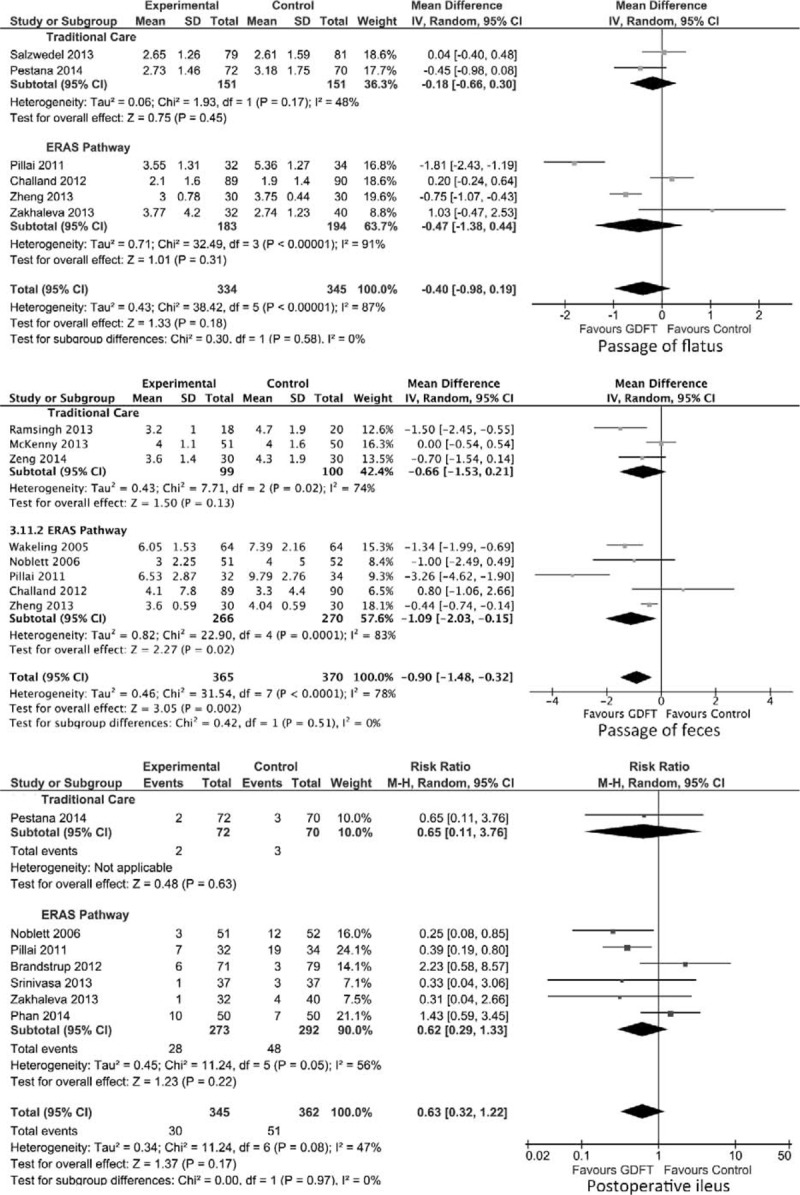
Results: A total of 23 studies were included with 2099 patients: 1040 who underwent GDFT and 1059 who received conventional fluid therapy. GDFT was associated with a significant reduction in morbidity (risk ratio [RR] 0.76, 95% confidence interval [CI] 0.66-0.89, P = 0.0007), hospital length of stay (LOS; mean difference -1.55 days, 95% CI -2.73 to -0.36, P = 0.01), intensive care LOS (mean difference -0.63 days, 95% CI -1.18 to -0.09, P = 0.02), and time to passage of feces (mean difference -0.90 days, 95% CI -1.48 to -0.32 days, P = 0.002). However, no difference was seen in mortality, return of flatus, or risk of paralytic ileus. If patients were managed in an ERAS pathway, the only significant reductions were in intensive care LOS (mean difference -0.63 days, 95% CI -0.94 to -0.32, P < 0.0001) and time to passage of feces (mean difference -1.09 days, 95% CI -2.03 to -0.15, P = 0.02). If managed in a traditional care setting, a significant reduction was seen in both overall morbidity (RR 0.69, 95% CI 0.57 to -0.84, P = 0.0002) and total hospital LOS (mean difference -2.14, 95% CI -4.15 to -0.13, P = 0.04).
Conclusions: GDFT may not be of benefit to all elective patients undergoing major abdominal surgery, particularly those managed in an ERAS setting.
Figures

References
-
- Giglio MT, Marucci M, Testini M, et al. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery: a meta-analysis of randomized controlled trials. Br J Anaesth 2009; 103:637–646. - PubMed
-
- Holland J, Carey M, Hughes N, et al. Intraoperative splanchnic hypoperfusion, increased intestinal permeability, down-regulation of monocyte class II major histocompatibility complex expression, exaggerated acute phase response, and sepsis. Am J Surg 2005; 190:393–400. - PubMed
-
- Bennett-Guerrero E, Welsby I, Dunn TJ, et al. The use of a postoperative morbidity survey to evaluate patients with prolonged hospitalization after routine, moderate-risk, elective surgery. Anesth Analg 1999; 89:514–519. - PubMed
-
- Funk DJ, Moretti EW, Gan TJ. Minimally invasive cardiac output monitoring in the perioperative setting. Anesth Analg 2009; 108:887–897. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
