

Contribution of APC and MUTYH mutations to familial adenomatous polyposis susceptibility in Hungary
- PMID: 26446593
- PMCID: PMC4698287
- DOI: 10.1007/s10689-015-9845-5
Contribution of APC and MUTYH mutations to familial adenomatous polyposis susceptibility in Hungary
Abstract
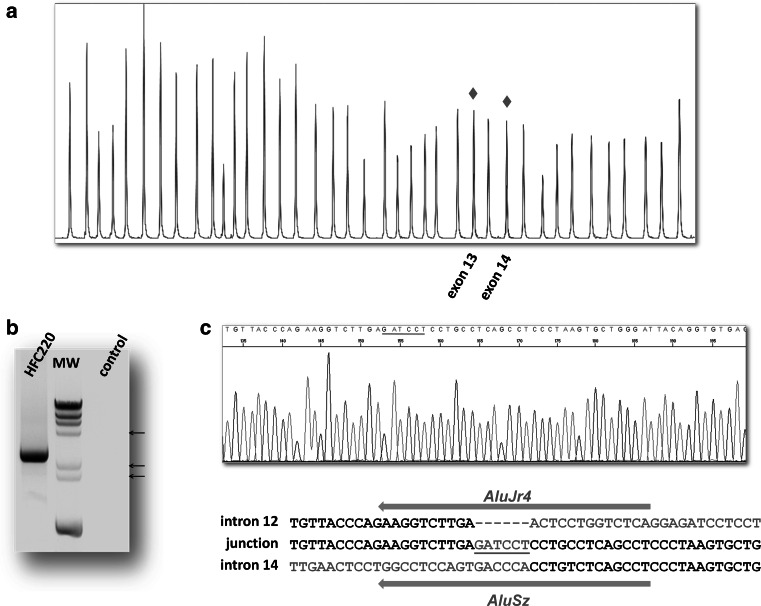
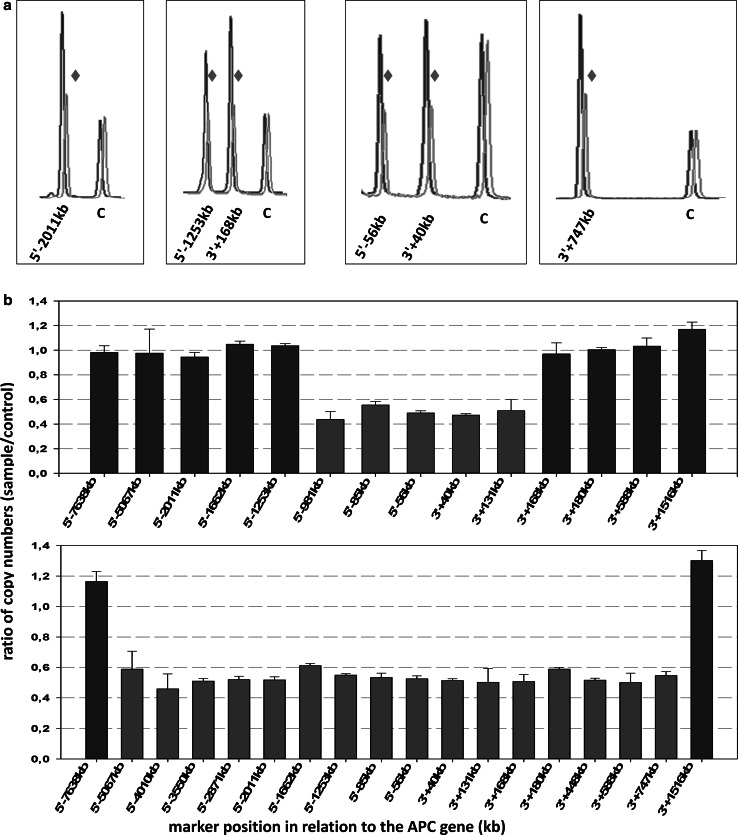
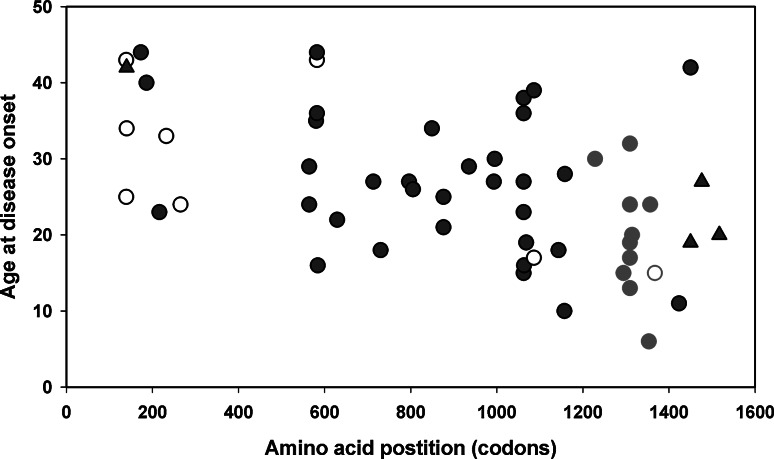
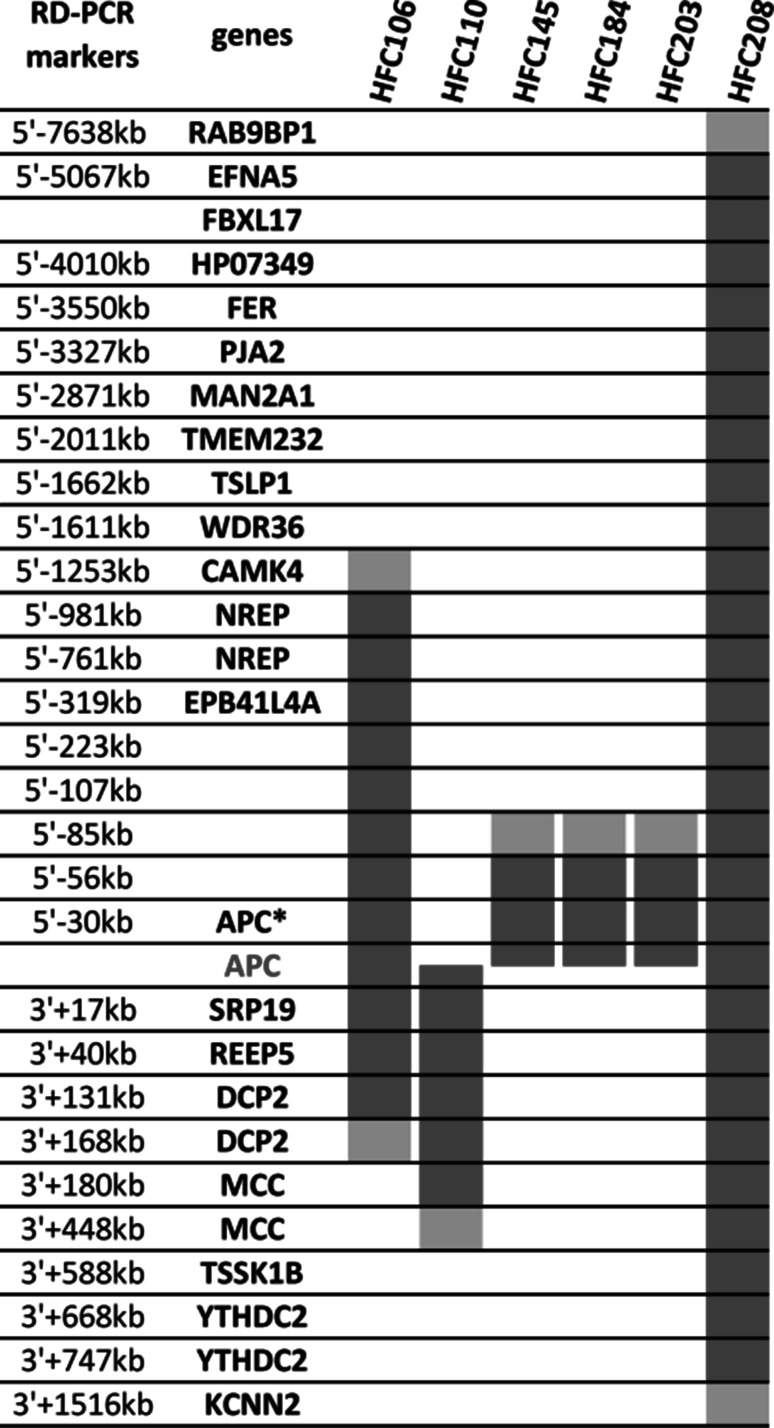
Familial adenomatous polyposis (FAP) is a colorectal cancer predisposition syndrome with considerable genetic and phenotypic heterogeneity, defined by the development of multiple adenomas throughout the colorectum. FAP is caused either by monoallelic mutations in the adenomatous polyposis coli gene APC, or by biallelic germline mutations of MUTYH, this latter usually presenting with milder phenotype. The aim of the present study was to characterize the genotype and phenotype of Hungarian FAP patients. Mutation screening of 87 unrelated probands from FAP families (21 of them presented as the attenuated variant of the disease, showing <100 polyps) was performed using DNA sequencing and multiplex ligation-dependent probe amplification. Twenty-four different pathogenic mutations in APC were identified in 65 patients (75 %), including nine cases (37.5 %) with large genomic alterations. Twelve of the point mutations were novel. In addition, APC-negative samples were also tested for MUTYH mutations and we were able to identify biallelic pathogenic mutations in 23 % of these cases (5/22). Correlations between the localization of APC mutations and the clinical manifestations of the disease were observed, cases with a mutation in the codon 1200-1400 region showing earlier age of disease onset (p < 0.003). There were only a few, but definitive dissimilarities between APC- and MUTYH-associated FAP in our cohort: the age at onset of polyposis was significantly delayed for biallelic MUTYH mutation carriers as compared to patients with an APC mutation. Our data represent the first comprehensive study delineating the mutation spectra of both APC and MUTYH in Hungarian FAP families, and underscore the overlap between the clinical characteristics of APC- and MUTYH-associated phenotypes, necessitating a more appropriate clinical characterization of FAP families.
Keywords: APC; Colorectal cancer; Familial adenomatous polyposis; Genotype–phenotype correlations; Germline mutations; MUTYH.
Figures
Similar articles
-
Clinical characterization and mutation spectrum in patients with familial adenomatous polyposis in China.J Gastroenterol Hepatol. 2019 Sep;34(9):1497-1503. doi: 10.1111/jgh.14704. Epub 2019 Jun 13. J Gastroenterol Hepatol. 2019. PMID: 31062380
-
Germline mutations in APC and MUTYH are responsible for the majority of families with attenuated familial adenomatous polyposis.Clin Genet. 2007 May;71(5):427-33. doi: 10.1111/j.1399-0004.2007.00766.x. Clin Genet. 2007. PMID: 17489848
-
Colorectal Adenomatous Polyposis: Heterogeneity of Susceptibility Gene Mutations and Phenotypes in a Cohort of Italian Patients.Genet Test Mol Biomarkers. 2016 Dec;20(12):777-785. doi: 10.1089/gtmb.2016.0198. Epub 2016 Oct 5. Genet Test Mol Biomarkers. 2016. PMID: 27705013
-
The genetics of familial adenomatous polyposis (FAP) and MutYH-associated polyposis (MAP).Acta Gastroenterol Belg. 2011 Sep;74(3):421-6. Acta Gastroenterol Belg. 2011. PMID: 22103048 Review.
-
MutYH-associated polyposis.Ter Arkh. 2019 Mar 18;91(2):97-100. doi: 10.26442/00403660.2019.02.000124. Ter Arkh. 2019. PMID: 31094179 Review.
Cited by
-
Complex Characterization of Germline Large Genomic Rearrangements of the BRCA1 and BRCA2 Genes in High-Risk Breast Cancer Patients-Novel Variants from a Large National Center.Int J Mol Sci. 2020 Jun 30;21(13):4650. doi: 10.3390/ijms21134650. Int J Mol Sci. 2020. PMID: 32629901 Free PMC article.
-
Pathogenic APC Variants in Latvian Familial Adenomatous Polyposis Patients.Medicina (Kaunas). 2019 Sep 20;55(10):612. doi: 10.3390/medicina55100612. Medicina (Kaunas). 2019. PMID: 31547110 Free PMC article.
-
Tumor suppressor genes in familial adenomatous polyposis.Gastroenterol Hepatol Bed Bench. 2017 Winter;10(1):3-13. Gastroenterol Hepatol Bed Bench. 2017. PMID: 28331559 Free PMC article. Review.
-
Three novel mutations of APC gene in Chinese patients with familial adenomatous polyposis.Tumour Biol. 2016 Aug;37(8):11421-7. doi: 10.1007/s13277-016-4986-1. Epub 2016 Mar 22. Tumour Biol. 2016. PMID: 27000756 Free PMC article.
-
Identification of Germline Mutations in Genes Involved in Classic FAP in Patients from Northern Brazil.Cancer Diagn Progn. 2022 May 3;2(3):405-410. doi: 10.21873/cdp.10123. eCollection 2022 May-Jun. Cancer Diagn Progn. 2022. PMID: 35530639 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
