

Treatment of Retinoblastoma: The Role of External Beam Radiotherapy
- PMID: 26446627
- PMCID: PMC4630033
- DOI: 10.3349/ymj.2015.56.6.1478
Treatment of Retinoblastoma: The Role of External Beam Radiotherapy
Abstract
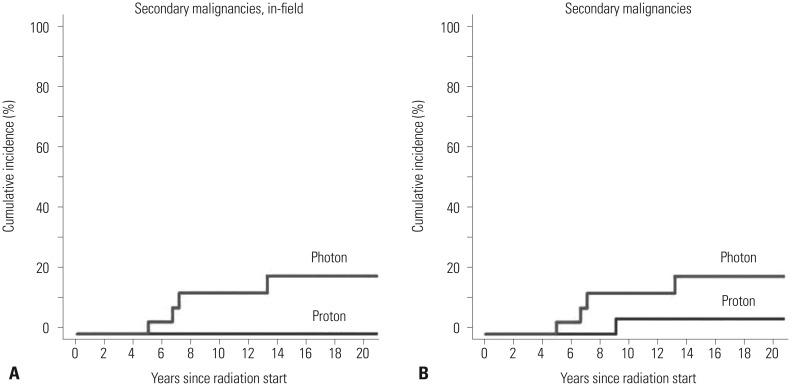
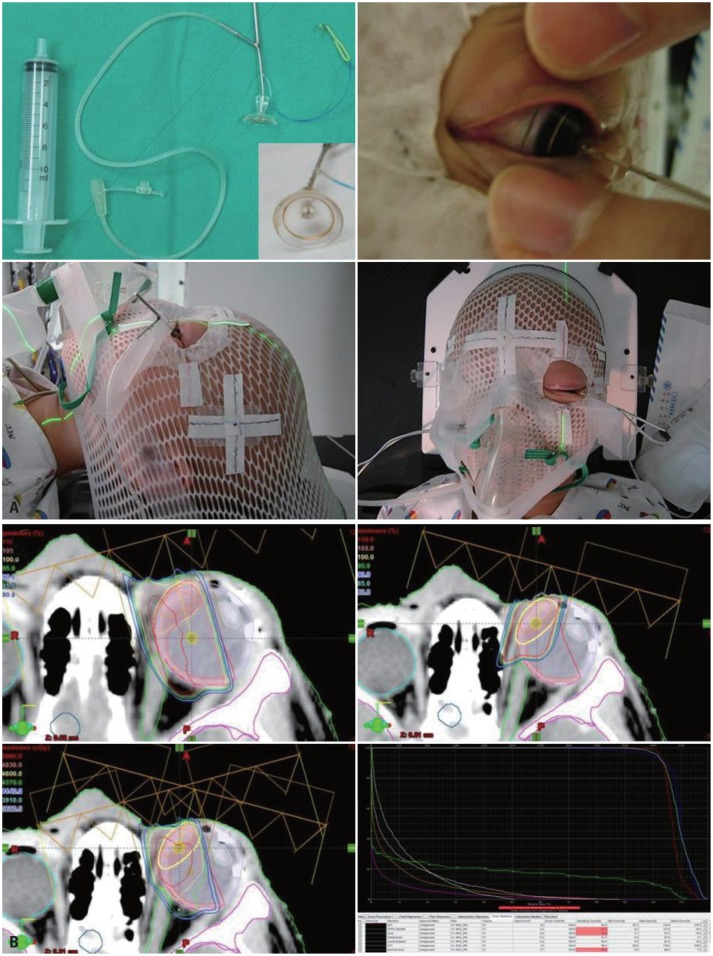
The risk of radiotherapy-related secondary cancers in children with constitutional retinoblastoma 1 (RB1) mutations has led to reduced use of external beam radiotherapy (EBRT) for RB. Presently, tumor reduction with chemotherapy with or without focal surgery (chemosurgery) is most commonly undertaken; EBRT is avoided as much as possible and is considered only as the last treatment option prior to enucleation. Nevertheless, approximately 80% of patients are diagnosed at a locally advanced stage, and only 20-25% of early stage RB patients can be cured with a chemosurgery strategy. As a whole, chemotherapy fails in more than two-thirds of eyes with advanced stage disease, requiring EBRT or enucleation. Radiotherapy is still considered necessary for patients with large tumor(s) who are not candidates for chemosurgery but who have visual potential. When radiation therapy is indicated, the lowest possible radiation dose combined with systemic or local chemotherapy and focal surgery may yield the best clinical outcomes in terms of local control and treatment-related toxicity. Proton beam therapy is one EBRT method that can be used for treatment of RB and reduces the radiation dose delivered to the adjacent orbital bone while maintaining an adequate dose to the tumor. To maximize the therapeutic success of treatment of advanced RB, the possibility of integrating radiotherapy at early stages of treatment may need to be discussed by a multidisciplinary team, rather than considering EBRT as only a last treatment option.
Keywords: Retinoblastoma; external beam radiotherapy; treatment.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures


References
-
- Halperin EC, Constine LS, Tarbell NJ, Kun LE. Pediatric Radiation Oncology. Philadelphia: Wolters Kluwer Health; 2012.
-
- Abramson DH. Retinoblastoma: saving life with vision. Annu Rev Med. 2014;65:171–184. - PubMed
-
- Munier FL, Verwey J, Pica A, Balmer A, Zografos L, Abouzeid H, et al. New developments in external beam radiotherapy for retinoblastoma: from lens to normal tissue-sparing techniques. Clin Experiment Ophthalmol. 2008;36:78–89. - PubMed
-
- Dimaras H, Kimani K, Dimba EA, Gronsdahl P, White A, Chan HS, et al. Retinoblastoma. Lancet. 2012;379:1436–1446. - PubMed
-
- Dimaras H, Dimba EA, Gallie BL. Challenging the global retinoblastoma survival disparity through a collaborative research effort. Br J Ophthalmol. 2010;94:1415–1416. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
