

Early Standard Electroencephalogram Abnormalities Predict Mortality in Septic Intensive Care Unit Patients
- PMID: 26447697
- PMCID: PMC4598037
- DOI: 10.1371/journal.pone.0139969
Early Standard Electroencephalogram Abnormalities Predict Mortality in Septic Intensive Care Unit Patients
Abstract
Introduction: Sepsis is associated with increased mortality, delirium and long-term cognitive impairment in intensive care unit (ICU) patients. Electroencephalogram (EEG) abnormalities occurring at the acute stage of sepsis may correlate with severity of brain dysfunction. Predictive value of early standard EEG abnormalities for mortality in ICU septic patients remains to be assessed.
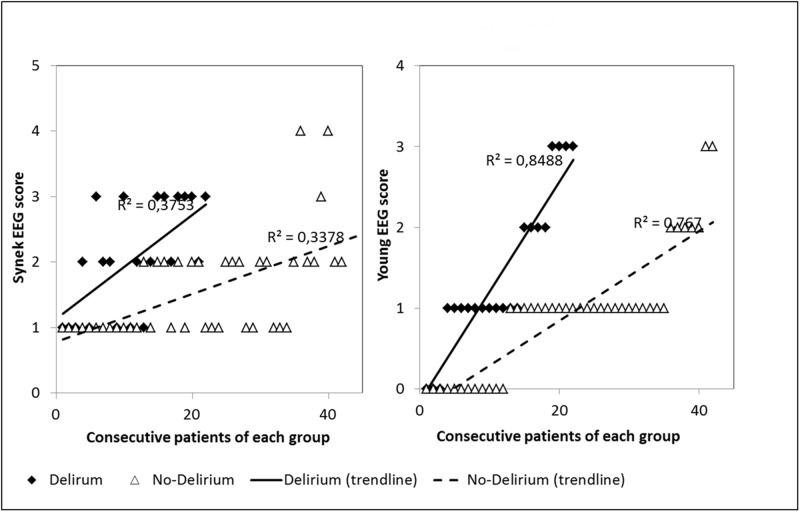
Methods: In this prospective, single center, observational study, standard EEG was performed, analyzed and classified according to both Synek and Young EEG scales, in consecutive patients acutely admitted in ICU for sepsis. Delirium, coma and the level of sedation were assessed at the time of EEG recording; and duration of sedation, occurrence of in-ICU delirium or death were assessed during follow-up. Adjusted analyses were carried out using multiple logistic regression.
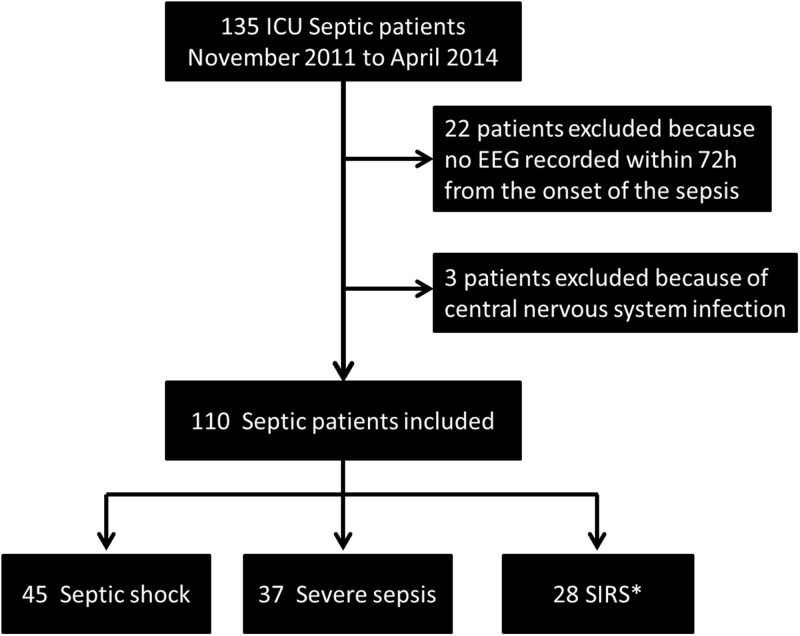
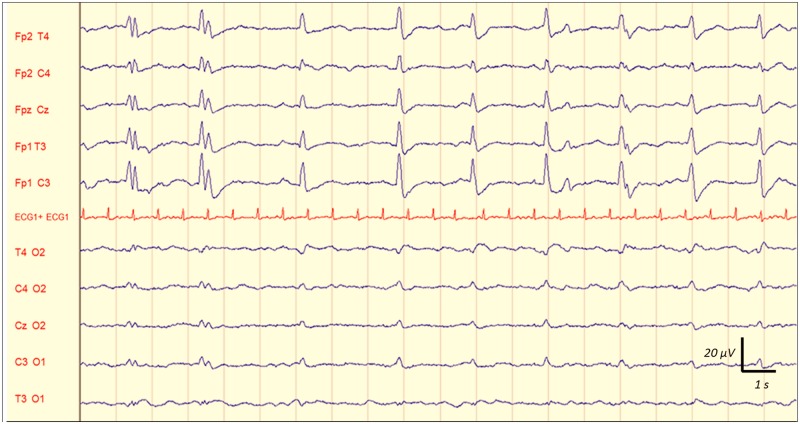
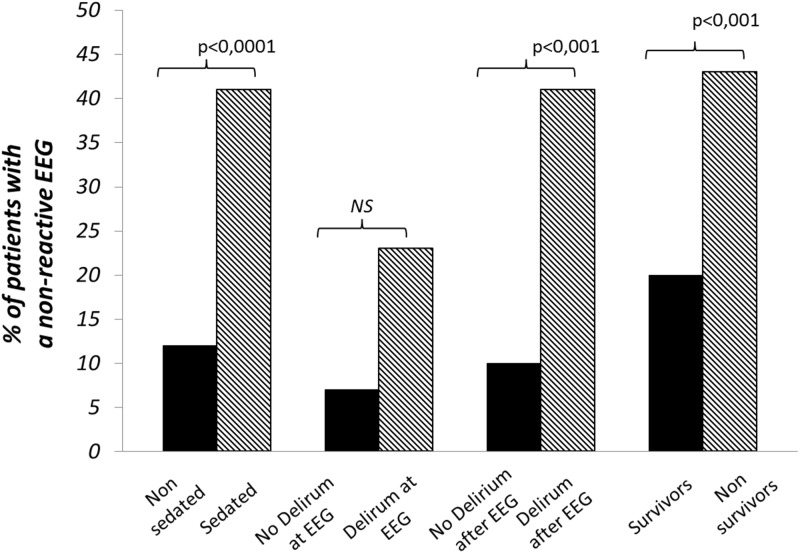
Results: One hundred ten patients were included, mean age 63.8 (±18.1) years, median SAPS-II score 38 (29-55). At the time of EEG recording, 46 patients (42%) were sedated and 22 (20%) suffered from delirium. Overall, 54 patients (49%) developed delirium, of which 32 (29%) in the days after EEG recording. 23 (21%) patients died in the ICU. Absence of EEG reactivity was observed in 27 patients (25%), periodic discharges (PDs) in 21 (19%) and electrographic seizures (ESZ) in 17 (15%). ICU mortality was independently associated with a delta-predominant background (OR: 3.36; 95% CI [1.08 to 10.4]), absence of EEG reactivity (OR: 4.44; 95% CI [1.37-14.3], PDs (OR: 3.24; 95% CI [1.03 to 10.2]), Synek grade ≥ 3 (OR: 5.35; 95% CI [1.66-17.2]) and Young grade > 1 (OR: 3.44; 95% CI [1.09-10.8]) after adjustment to Simplified Acute Physiology Score (SAPS-II) at admission and level of sedation. Delirium at the time of EEG was associated with ESZ in non-sedated patients (32% vs 10%, p = 0.037); with Synek grade ≥ 3 (36% vs 7%, p< 0.05) and Young grade > 1 (36% vs 17%, p< 0.001). Occurrence of delirium in the days after EEG was associated with a delta-predominant background (48% vs 15%, p = 0.001); absence of reactivity (39% vs 10%, p = 0.003), Synek grade ≥ 3 (42% vs 17%, p = 0.001) and Young grade >1 (58% vs 17%, p = 0.0001).
Conclusions: In this prospective cohort of 110 septic ICU patients, early standard EEG was significantly disturbed. Absence of EEG reactivity, a delta-predominant background, PDs, Synek grade ≥ 3 and Young grade > 1 at day 1 to 3 following admission were independent predictors of ICU mortality and were associated with occurence of delirium. ESZ and PDs, found in about 20% of our patients. Their prevalence could have been higher, with a still higher predictive value, if they had been diagnosed more thoroughly using continuous EEG.
Conflict of interest statement
Figures
References
-
- Eidelman LA, Putterman D, Putterman C, Sprung CL (1996) The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA 275: 470–473. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
