

Analysis of 24-Hour Ambulatory Blood Pressure Monitoring in Children With Obstructive Sleep Apnea: A Hospital-Based Study
- PMID: 26448004
- PMCID: PMC4616740
- DOI: 10.1097/MD.0000000000001568
Analysis of 24-Hour Ambulatory Blood Pressure Monitoring in Children With Obstructive Sleep Apnea: A Hospital-Based Study
Abstract
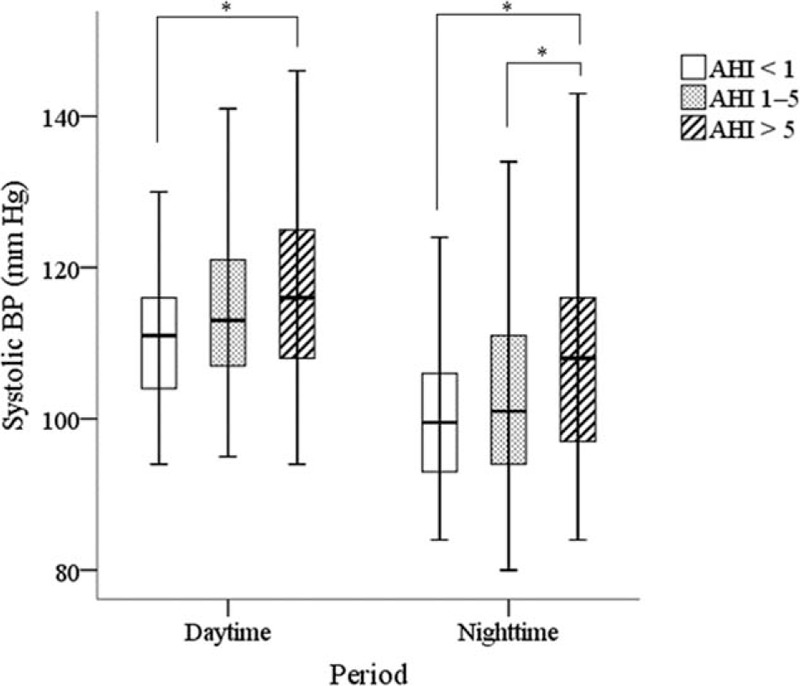
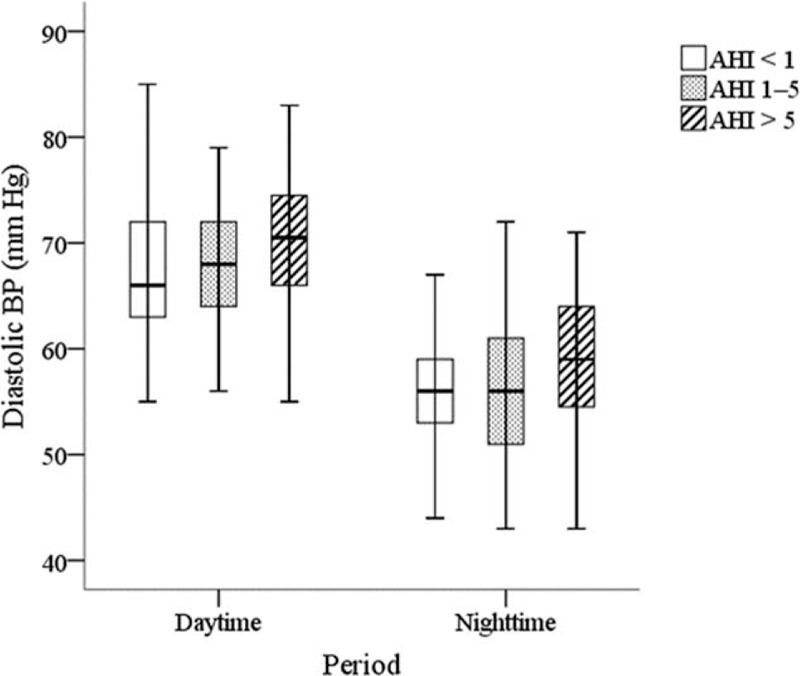
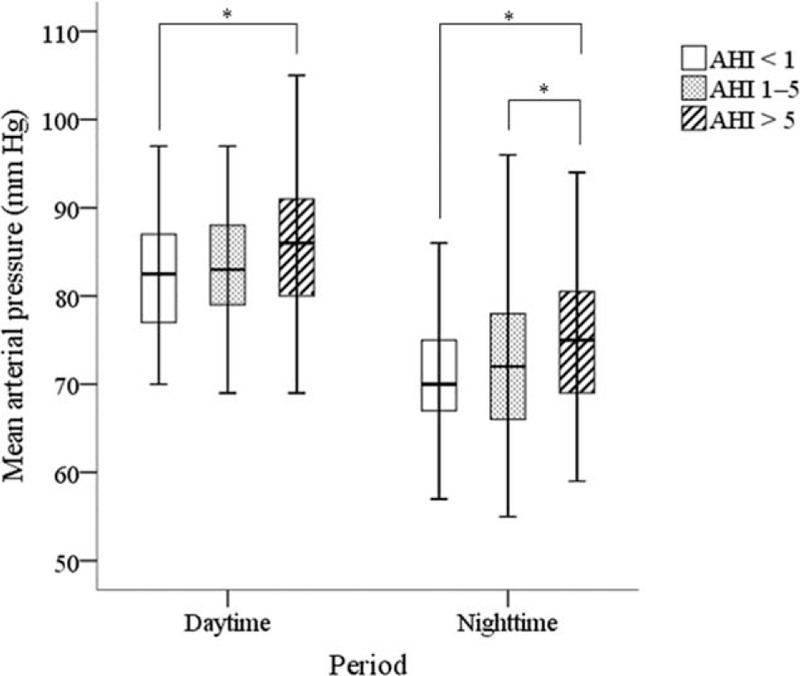
In the present study, we aimed to verify associations between ambulatory blood pressure (ABP) and pediatric obstructive sleep apnea (OSA) in a hospital-based population. This was a cross-sectional observational study on children aged 4 to 16 years with OSA-related symptoms from a tertiary referral medical center. All children received overnight polysomnography and 24-hour recording of ABP. Severity of the disease was classified as primary snoring (apnea-hypopnea index, AHI <1), mild OSA (AHI 1-5), and moderate-to-severe OSA (AHI >5). For 195 children enrolled in this study (mean age, 7.8 ± 3.4 years; 69% boy), ABP increased as severity of OSA increased. During daytime, children with moderate-to-severe OSA had significantly higher systolic blood pressure (BP) (117.0 ± 12.7 vs 110.5 ± 9.3 mmHg), mean arterial pressure (MAP) (85.6 ± 8 .1 vs 81.6 ± 6.8 mmHg), and diastolic BP load (12.0 ± 9.6 vs 8.4 ± 10.9 mmHg) compared with children with primary snoring. During nighttime, children with moderate-to-severe OSA had significantly higher systolic BP (108.6 ± 15.0 vs 100.0 ± 9.4 mmHg), MAP (75.9 ± 9.6 vs 71.1 ± 7.0 mmHg), systolic BP load (44.0 ± 32.6 vs 26.8 ± 24.5 mmHg), systolic BP index (0.5 ± 13.1 vs -6.8 ± 8.5 mmHg), and higher prevalence of systolic hypertension (47.6% vs 14.7 %) compared with children with primary snoring. Multiple linear regression analyses revealed an independent association between AHI and nighttime systolic BP and MAP after adjusting for adiposity variables. This large hospital-based study showed that children with moderate-to-severe OSA had a higher ABP compared with children who were primary snorers. As elevated BP in childhood predicts future cardiovascular risks, children with severe OSA should be treated properly to prevent further adverse cardiovascular outcomes.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
24-Hour Ambulatory Blood Pressure Variability in Children with Obstructive Sleep Apnea.Laryngoscope. 2021 Sep;131(9):2126-2132. doi: 10.1002/lary.29455. Epub 2021 Feb 18. Laryngoscope. 2021. PMID: 33599298
-
Office Blood Pressure Monitoring in Children with Obesity and Obstructive Sleep Apnea.J Pediatr. 2022 Jul;246:138-144.e2. doi: 10.1016/j.jpeds.2022.03.024. Epub 2022 Mar 18. J Pediatr. 2022. PMID: 35314156
-
Comparisons of Office and 24-Hour Ambulatory Blood Pressure Monitoring in Children with Obstructive Sleep Apnea.J Pediatr. 2017 Mar;182:177-183.e2. doi: 10.1016/j.jpeds.2016.11.032. Epub 2016 Dec 6. J Pediatr. 2017. PMID: 27939257
-
Blood Pressure Regulation and Hypertension in Obstructive Sleep Apnea Syndrome: A Historical Perspective.Intern Med. 2024 Dec 1;63(23):3131-3136. doi: 10.2169/internalmedicine.2960-23. Epub 2024 Apr 16. Intern Med. 2024. PMID: 38631858 Free PMC article. Review.
-
Effect of Sleep Disturbances on Blood Pressure.Hypertension. 2021 Apr;77(4):1036-1046. doi: 10.1161/HYPERTENSIONAHA.120.14479. Epub 2021 Feb 22. Hypertension. 2021. PMID: 33611935 Free PMC article. Review.
Cited by
-
Does obstructive sleep apnoea contribute to obesity, hypertension and kidney dysfunction in children? A systematic review protocol.BMJ Open. 2020 Aug 30;10(8):e039342. doi: 10.1136/bmjopen-2020-039342. BMJ Open. 2020. PMID: 32868367 Free PMC article.
-
Prevalence of High Blood Pressure in Pediatric Patients with Sleep-Disordered Breathing, Reversibility after Treatment: The KIDS TRIAL Study Protocol.Children (Basel). 2022 Nov 28;9(12):1849. doi: 10.3390/children9121849. Children (Basel). 2022. PMID: 36553294 Free PMC article.
-
A "Wear and Tear" Hypothesis to Explain Sudden Infant Death Syndrome.Front Neurol. 2016 Oct 28;7:180. doi: 10.3389/fneur.2016.00180. eCollection 2016. Front Neurol. 2016. PMID: 27840622 Free PMC article.
-
Ambulatory Blood Pressure Monitoring in Pediatrics.Curr Hypertens Rep. 2019 Jul 26;21(9):71. doi: 10.1007/s11906-019-0976-1. Curr Hypertens Rep. 2019. PMID: 31350605 Review.
-
The Use of Ambulatory Blood Pressure Monitoring As Standard of Care in Pediatrics.Front Pediatr. 2017 Jun 30;5:153. doi: 10.3389/fped.2017.00153. eCollection 2017. Front Pediatr. 2017. PMID: 28713799 Free PMC article. Review.
References
-
- Marcus CL, Brooks LJ, Draper KA, et al. American Academy of Pediatrics Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012; 130:e714–e755. - PubMed
-
- Kang KT, Lee PL, Weng WC, et al. Body weight status and obstructive sleep apnea in children. Int J Obes (Lond) 2012; 36:920–924. - PubMed
-
- Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000; 342:1378–1384. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005; 353:2034–2041. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
