

Risk Adjusting Survival Outcomes in Hospitals That Treat Patients With Cancer Without Information on Cancer Stage
- PMID: 26448610
- PMCID: PMC5038982
- DOI: 10.1001/jamaoncol.2015.3151
Risk Adjusting Survival Outcomes in Hospitals That Treat Patients With Cancer Without Information on Cancer Stage
Erratum in
-
Data Errors in Table.JAMA Oncol. 2015 Dec;1(9):1323. doi: 10.1001/jamaoncol.2015.5375. JAMA Oncol. 2015. PMID: 26659196 No abstract available.
Abstract
Importance: Instituting widespread measurement of outcomes for cancer hospitals using administrative data is difficult owing to lack of cancer-specific information such as disease stage.
Objective: To evaluate the performance of hospitals that treat patients with cancer using Medicare data for outcome ascertainment and risk adjustment and to assess whether hospital rankings based on these measures are altered by the addition of cancer-specific information.
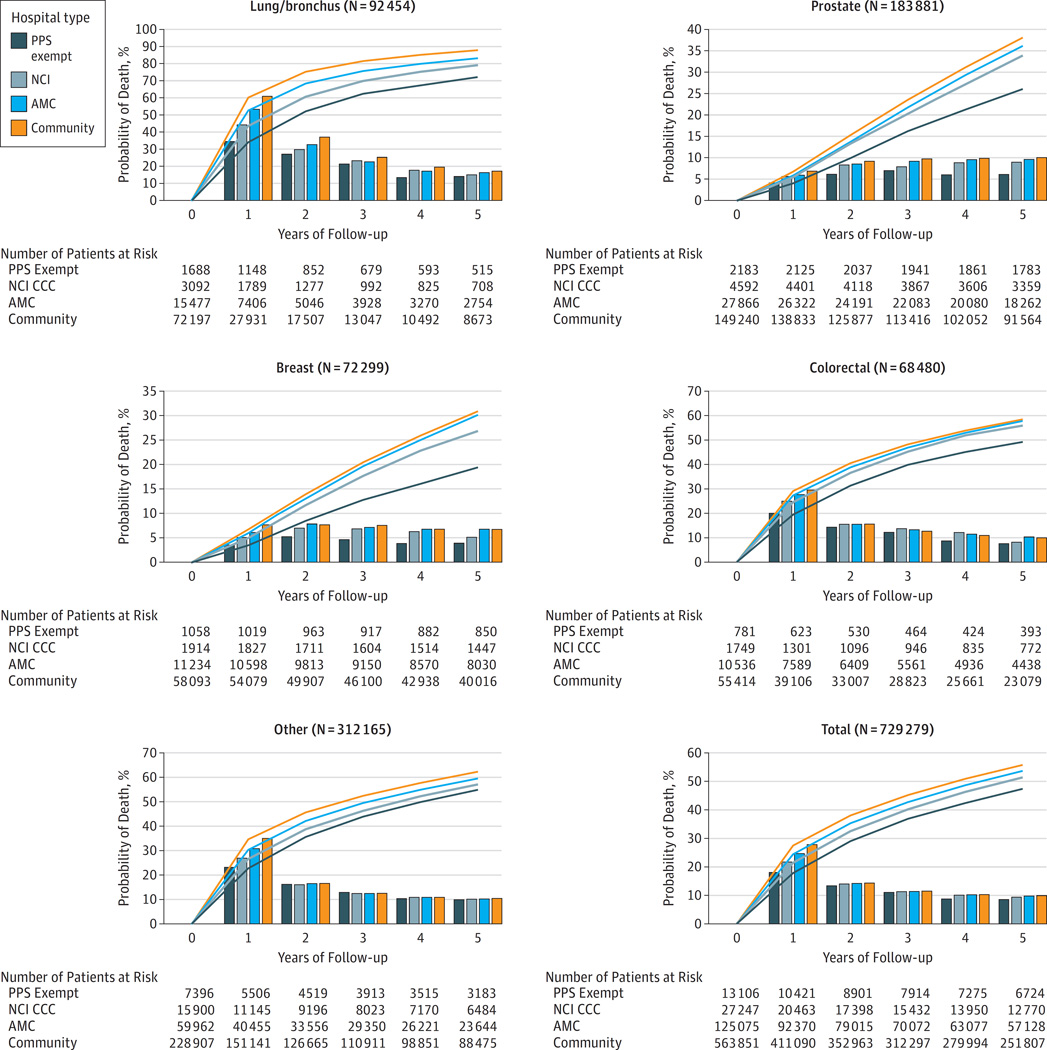
Design, setting, and participants: Risk-adjusted cumulative mortality rates of patients with cancer were captured in Medicare claims data from 2005 through 2009 nationally and assessed at the hospital level. Similar analyses were conducted using Surveillance, Epidemiology, and End Results (SEER)-Medicare data for the subset of the United States covered by the SEER program to determine whether the inclusion of cancer-specific information (only available in cancer registries) in risk adjustment altered measured hospital performance. Data were from 729 279 fee-for-service Medicare beneficiaries treated for cancer in 2006 at hospitals treating 10 or more patients with each of the following cancers, according to Medicare claims: lung, prostate, breast, colon, and other. An additional sample of 18 677 similar patients were included from the SEER-Medicare administrative data.
Main outcomes and measures: Risk-adjusted mortality overall and by cancer category, stratified by type of hospital; measures of correlation and agreement between hospital-level outcomes risk adjusted using Medicare data alone and Medicare data with SEER data.
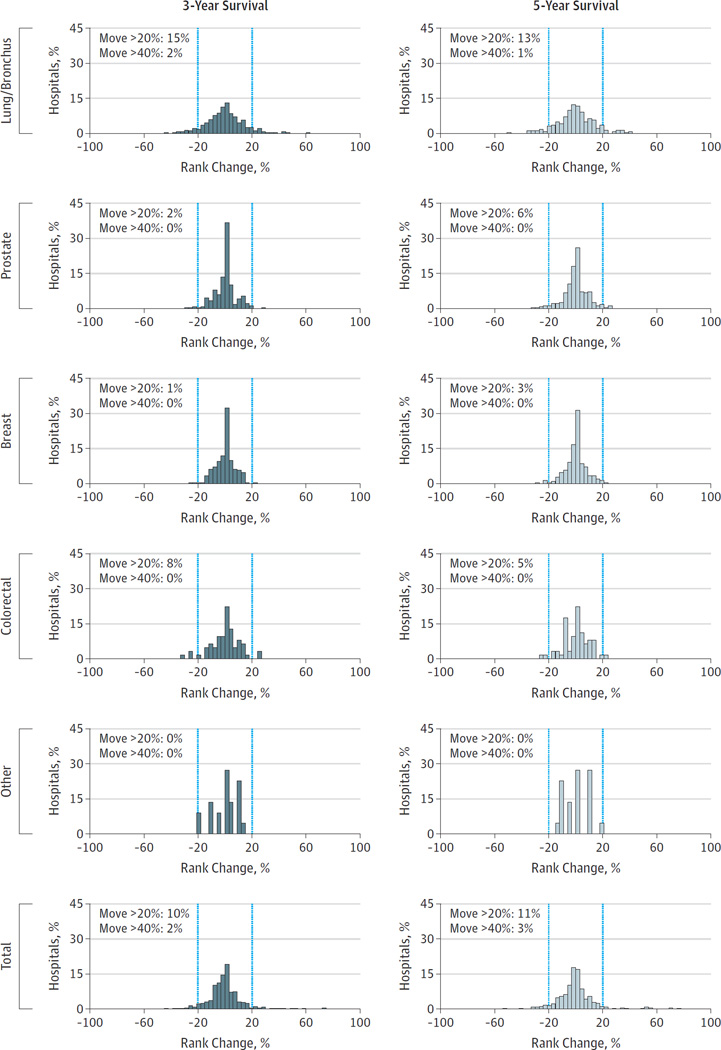
Results: There were large survival differences between different types of hospitals that treat Medicare patients with cancer. At 1 year, mortality for patients treated by hospitals exempt from the Medicare prospective payment system was 10% lower than at community hospitals (18% vs 28%) across all cancers, and the pattern persisted through 5 years of follow-up and within specific cancer categories. Performance ranking of hospitals was consistent with or without SEER-Medicare disease stage information (weighted κ ≥ 0.81).
Conclusions and relevance: Potentially important outcome differences exist between different types of hospitals that treat patients with cancer after risk adjustment using information in Medicare administrative data. This type of risk adjustment may be adequate for evaluating hospital performance, since the additional adjustment for data available only in cancer registries does not seem to appreciably alter measures of performance.
Conflict of interest statement
Disclosures: All authors are employed by a PPS-exempt cancer hospital, Memorial Sloan Kettering Cancer Center. No other conflicts are reported.
Figures
References
-
- Murphy SL, Xu J, Kochanek KD. Deaths: final data for 2010. National vital statistics reports. 2013;61(4):1–118. - PubMed
-
- Birkmeyer NJ, Goodney PP, Stukel TA, Hillner BE, Birkmeyer JD. Do cancer centers designated by the National Cancer Institute have better surgical outcomes? Cancer. 2005 Feb 1;103(3):435–441. - PubMed
-
- Cheung MC, Hamilton K, Sherman R, et al. Impact of teaching facility status and high-volume centers on outcomes for lung cancer resection: an examination of 13,469 surgical patients. Ann Surg Oncol. 2009 Jan;16(1):3–13. - PubMed
-
- Petitti D, Hewitt M. Interpreting the volume-outcome relationship in the context of cancer care. National Academies Press; 2001. - PubMed
-
- Clough JD, Patel K, Riley GF, Rajkumar R, Conway PH, Bach PB. Wide variation in payments for medicare beneficiary oncology services suggests room for practice-level improvement. Health Aff (Millwood) 2015 Apr 1;34(4):601–608. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
