

Is dying in hospital better than home in incurable cancer and what factors influence this? A population-based study
- PMID: 26449231
- PMCID: PMC4599664
- DOI: 10.1186/s12916-015-0466-5
Is dying in hospital better than home in incurable cancer and what factors influence this? A population-based study
Abstract
Background: Studies show that most patients with advanced cancer prefer to die at home. However, not all have equal chances and the evidence is unclear on whether dying at home is better. This study aims to determine the association between place of death, health services used, and pain, feeling at peace, and grief intensity.
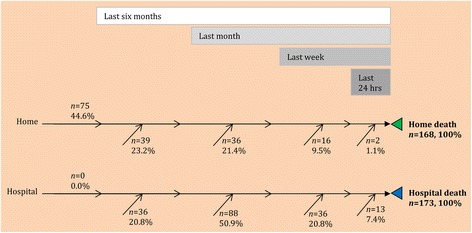
Methods: Mortality follow-back study of 352 cancer patients who died in hospital (n = 177) or at home (n = 175) in London, UK. Bereaved relatives identified from death registrations completed a questionnaire including validated measures of patient's pain and peace in the last week of life and their own grief intensity. We determined factors influencing death at home, and associations between place of death and pain, peace, and grief.
Results: Where people died was, for most (80%), the place where they lived during their last week of life. Four factors explained >91% of home deaths: patient's preference, relative's preference, home palliative care, or district/community nursing. The propensity of death at home also increased when the relative was aware of incurability and the patient discussed his/her preferences with family. Dying in hospital was associated with more hospital days, fewer general practitioner (GP) home visits, and fewer days taken off work by relatives. Adjusting for confounders, patients who died at home experienced similar pain levels but more peace in their last week of life (ordered log odds ratio 0.69, P = 0.007). Grief was less intense for their relatives than for those of patients who died in hospital (β, -0.15 around time of death and -0.14 at questionnaire completion, P = 0.02).
Conclusion: The study suggests that dying at home is better than hospital for peace and grief, but requires a discussion of preferences, GP home visits, and relatives to be given time off work.
Trial registration: National Institute of Health Research (NIHR) Clinical Research Network Portfolio. UKCRN7041.
Figures


Comment in
-
Home death versus hospital death: are they comparable at all?Evid Based Nurs. 2016 Jul;19(3):94. doi: 10.1136/ebnurs-2015-102287. Epub 2016 Apr 7. Evid Based Nurs. 2016. PMID: 27056840 No abstract available.
References
-
- Gomes B, Higginson IJ, Calanzani N, Cohen J, Deliens L, Daveson BA, et al. Preferences for place of death if faced with advanced cancer: a population survey in England, Flanders, Germany, Italy, The Netherlands, Portugal and Spain. Ann Oncol. 2012;23:2006–2015. doi: 10.1093/annonc/mdr602. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
