

Obstetric Anaesthetists' Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics
- PMID: 26449292
- PMCID: PMC4606761
- DOI: 10.1111/anae.13260
Obstetric Anaesthetists' Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics
Abstract
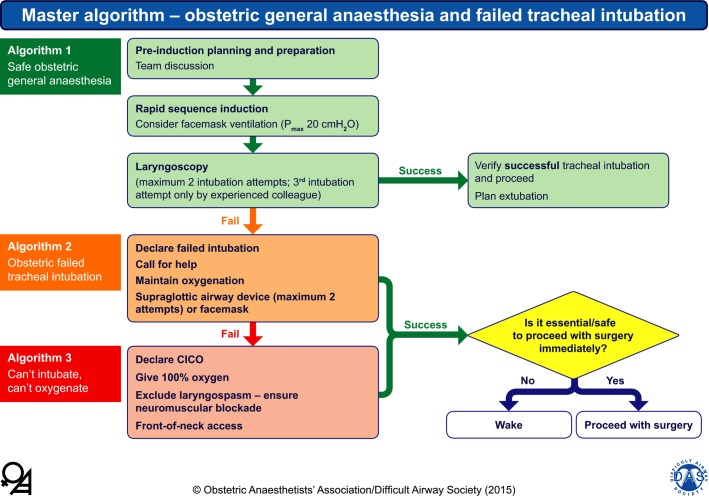
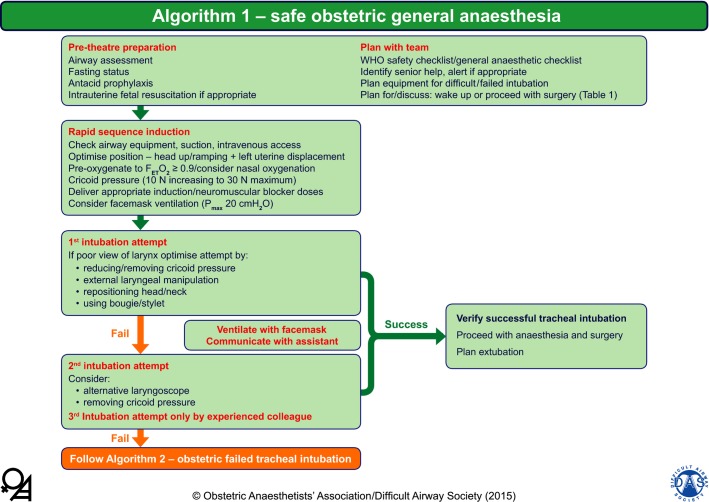
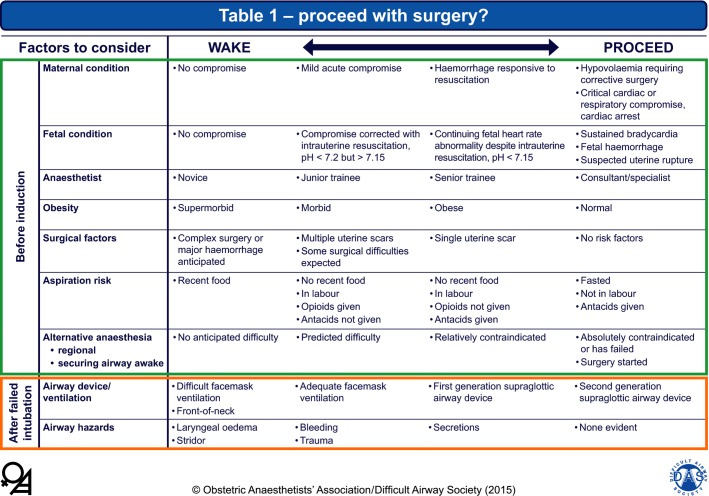
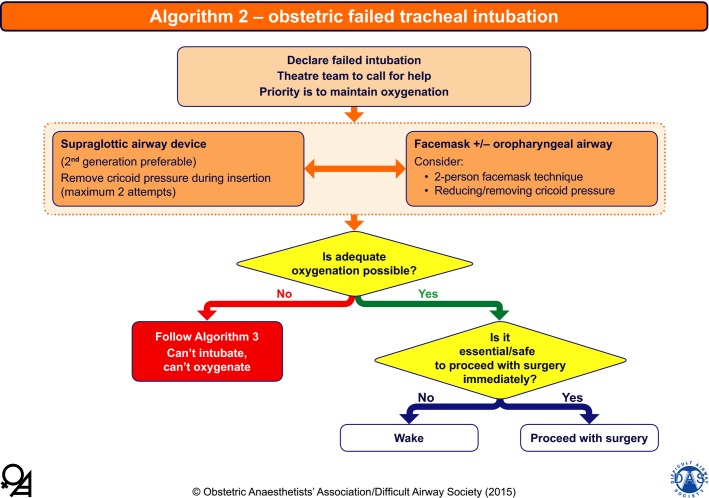
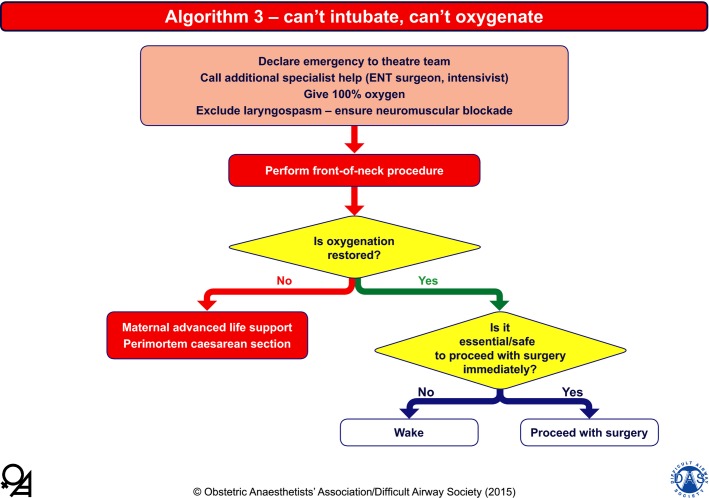
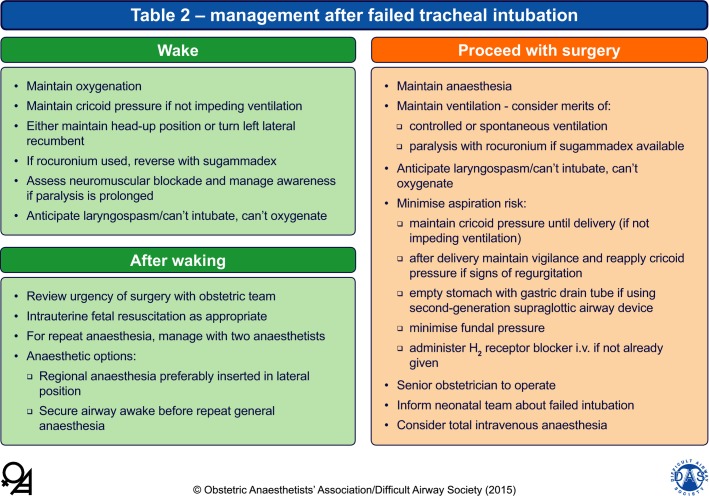
The Obstetric Anaesthetists' Association and Difficult Airway Society have developed the first national obstetric guidelines for the safe management of difficult and failed tracheal intubation during general anaesthesia. They comprise four algorithms and two tables. A master algorithm provides an overview. Algorithm 1 gives a framework on how to optimise a safe general anaesthetic technique in the obstetric patient, and emphasises: planning and multidisciplinary communication; how to prevent the rapid oxygen desaturation seen in pregnant women by advocating nasal oxygenation and mask ventilation immediately after induction; limiting intubation attempts to two; and consideration of early release of cricoid pressure if difficulties are encountered. Algorithm 2 summarises the management after declaring failed tracheal intubation with clear decision points, and encourages early insertion of a (preferably second-generation) supraglottic airway device if appropriate. Algorithm 3 covers the management of the 'can't intubate, can't oxygenate' situation and emergency front-of-neck airway access, including the necessity for timely perimortem caesarean section if maternal oxygenation cannot be achieved. Table 1 gives a structure for assessing the individual factors relevant in the decision to awaken or proceed should intubation fail, which include: urgency related to maternal or fetal factors; seniority of the anaesthetist; obesity of the patient; surgical complexity; aspiration risk; potential difficulty with provision of alternative anaesthesia; and post-induction airway device and airway patency. This decision should be considered by the team in advance of performing a general anaesthetic to make a provisional plan should failed intubation occur. The table is also intended to be used as a teaching tool to facilitate discussion and learning regarding the complex nature of decision-making when faced with a failed intubation. Table 2 gives practical considerations of how to awaken or proceed with surgery. The background paper covers recommendations on drugs, new equipment, teaching and training.
© 2015 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists of Great Britain and Ireland.
Figures
Comment in
-
Obstetric tracheal intubation guidelines and cricoid pressure.Anaesthesia. 2016 Mar;71(3):345-6. doi: 10.1111/anae.13382. Anaesthesia. 2016. PMID: 26864006 No abstract available.
-
Obstetric tracheal intubation guidelines and cricoid pressure--a reply.Anaesthesia. 2016 Mar;71(3):346-7. doi: 10.1111/anae.13394. Anaesthesia. 2016. PMID: 26864007 No abstract available.
-
High-flow humidified nasal pre-oxygenation in pregnant women.Anaesthesia. 2016 Jul;71(7):851-2. doi: 10.1111/anae.13533. Anaesthesia. 2016. PMID: 27291606 No abstract available.
References
-
- Henderson JJ, Popat MT, Latto IP, Pearce AC. Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia. 2004;59:675–94. - PubMed
-
- Apfelbaum JL, Hagberg CA, Caplan RA, et al. Practice Guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118:251–70. - PubMed
-
- American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Practice guidelines for obstetric anesthesia: an updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology. 2007;106:843–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
