

The role of clinically-relevant parameters on the cohesiveness of sclerosing foams in a biomimetic vein model
- PMID: 26449448
- PMCID: PMC4598354
- DOI: 10.1007/s10856-015-5587-z
The role of clinically-relevant parameters on the cohesiveness of sclerosing foams in a biomimetic vein model
Abstract
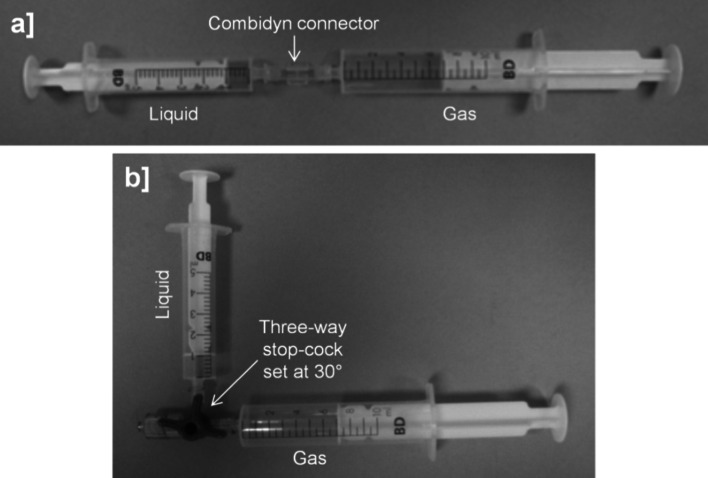
We have recently reported on the development of a biomimetic vein model to measure the performance of sclerosing foams. In this study we employed the model to compare the commercially-available Varithena(®) (polidocanol injectable foam) 1% varicose vein treatment (referred to as polidocanol endovenous microfoam, or PEM) with physician compounded foams (PCFs) made using different foam generation methods (Double Syringe System and Tessari methods) and different foam formulations [liquid to gas ratios of 1:3 or 1:7; gas mixtures composed of 100% CO2, various CO2:O2 mixtures and room air (RA)]. PCFs produced using the DSS method had longer dwell times (DTs) (range 0.54-2.21 s/cm in the 4 mm diameter vein model) than those of the corresponding PCFs produced by the Tessari technique (range 0.29-0.94 s/cm). PEM had the longest DT indicating the best cohesive stability of any of the foams produced (2.92 s/cm). Other biomimetic model variables investigated included effect of vessel size, delayed injection and rate of plug formation (injection speed). When comparing the 4 and 10 mm vessel diameters, the DTs seen in the 10 mm vessel were higher than those observed for the 4 mm vessel, as the vein angle had been reduced to 5° to allow for foam plug formation. PCF foam performance was in the order RA > CO2:O2 (35:65) ≅ CO2:O2 (65:35) > CO2; PEM had a longer DT than all PCFs (22.10 s/cm) except that for RA made by DSS which was similar but more variable. The effect of delayed injection was also investigated and the DT for PEM remained the longest of all foams with the lowest percentage deviation with respect to the mean values, indicating a consistent foam performance. When considering rate of plug formation, PEM consistently produced the longest DTs and this was possible even at low plug expansion rates (mean 29.5 mm/s, minimum 20.9 mm/s). The developed vein model has therefore demonstrated that PEM consistently displays higher foam stability and cohesiveness when compared to PCFs, over a range of clinically-relevant operational variables.
Figures







References
-
- Van den Oever R, Hepp B, Debbaut B, Simon I. Socio-economic impact of chronic venous insufficiency: an underestimated public health problem. Int Angiol. 1998;17(3):161–167. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
