

Increase of PD-L1 expressing B-precursor ALL cells in a patient resistant to the CD19/CD3-bispecific T cell engager antibody blinatumomab
- PMID: 26449653
- PMCID: PMC4599591
- DOI: 10.1186/s13045-015-0213-6
Increase of PD-L1 expressing B-precursor ALL cells in a patient resistant to the CD19/CD3-bispecific T cell engager antibody blinatumomab
Abstract
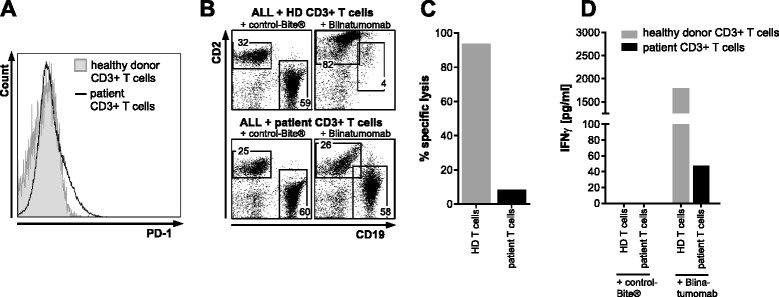
The bispecific T cell engager blinatumomab has shown encouraging clinical activity in B-precursor acute lymphoblastic leukemia (ALL). However, about half of relapsed/refractory patients do not respond to therapy. Here, we present the case of a 32-year-old male patient with refractory B-precursor ALL who was resistant to treatment with blinatumomab. Bone marrow immunohistochemistry revealed T cell infiltrates and an increase in programmed death-ligand 1 (PD-L1)-positive ALL cells as a potential immune escape mechanism. We were able to recapitulate the clinical observation in vitro by showing that blinatumomab was not able to mediate cytotoxicity of CD19-positive ALL cells using autologous T cells. In contrast, the addition of healthy donor T cells led to lysis of ALL cells.These results strongly encourage further systematic evaluation of checkpoint molecules in cases of blinatumomab treatment failure and might highlight a possible mechanism to overcome resistance to this otherwise highly effective treatment.
Figures

References
-
- Topp MS, Gökbuget N, Stein AS, Zugmaier G, O'Brien S, Bargou RC, et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: a multicentre, single-arm, phase 2 study. Lancet Oncol. 2014;16(1):57–66. doi: 10.1016/S1470-2045(14)71170-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
