

Diagnostic Impact of Bone-Subtraction CT Angiography for Patients with Acute Subarachnoid Hemorrhage
- PMID: 26450538
- PMCID: PMC7959933
- DOI: 10.3174/ajnr.A4497
Diagnostic Impact of Bone-Subtraction CT Angiography for Patients with Acute Subarachnoid Hemorrhage
Abstract
Background and purpose: Detection and evaluation of ruptured aneurysms is critical for choosing an appropriate endovascular or neurosurgical intervention. Our aim was to assess whether bone-subtraction CTA is capable of guiding treatment for cerebral aneurysms in patients with acute SAH and could replace DSA.
Materials and methods: We prospectively studied 116 consecutive patients with SAH with 16-detector row bone-subtraction CTA and DSA before intracranial aneurysm treatment. Two independent neuroradiologists reviewed the bone-subtraction CTA blinded to DSA (reference standard). We determined the accuracy of bone-subtraction CTA for aneurysm detection and the measurement of aneurysm dimensions and compared the radiation doses of the 2 imaging modalities.
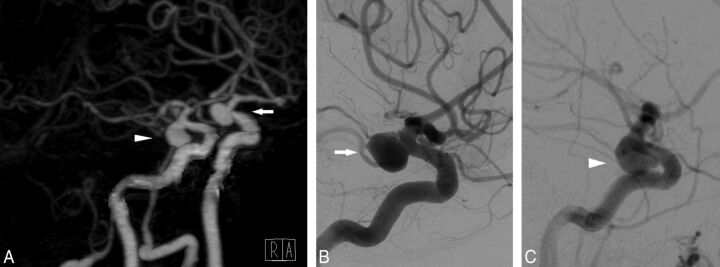
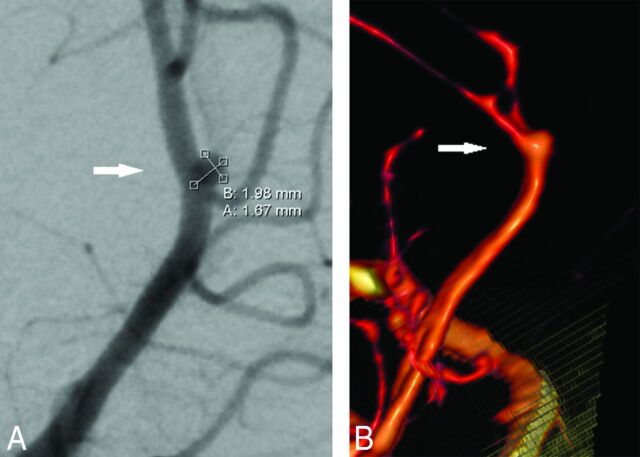
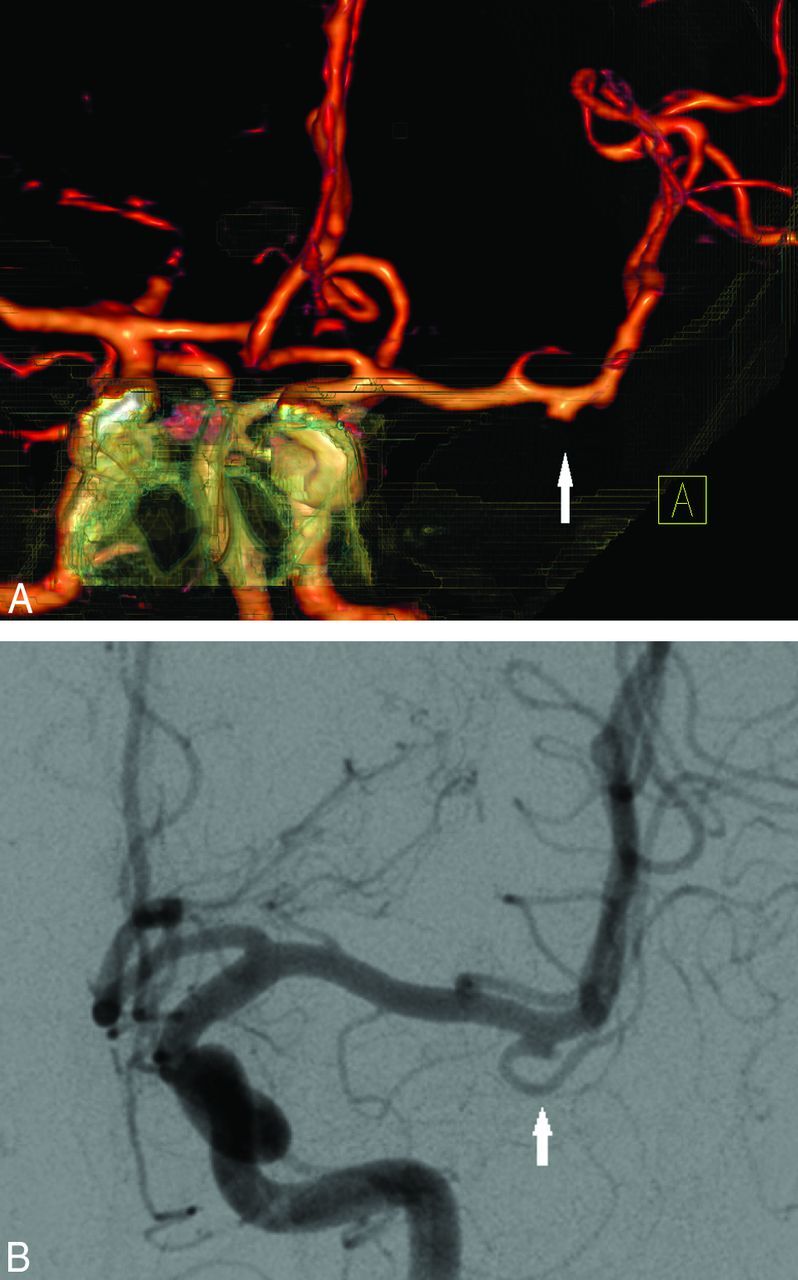
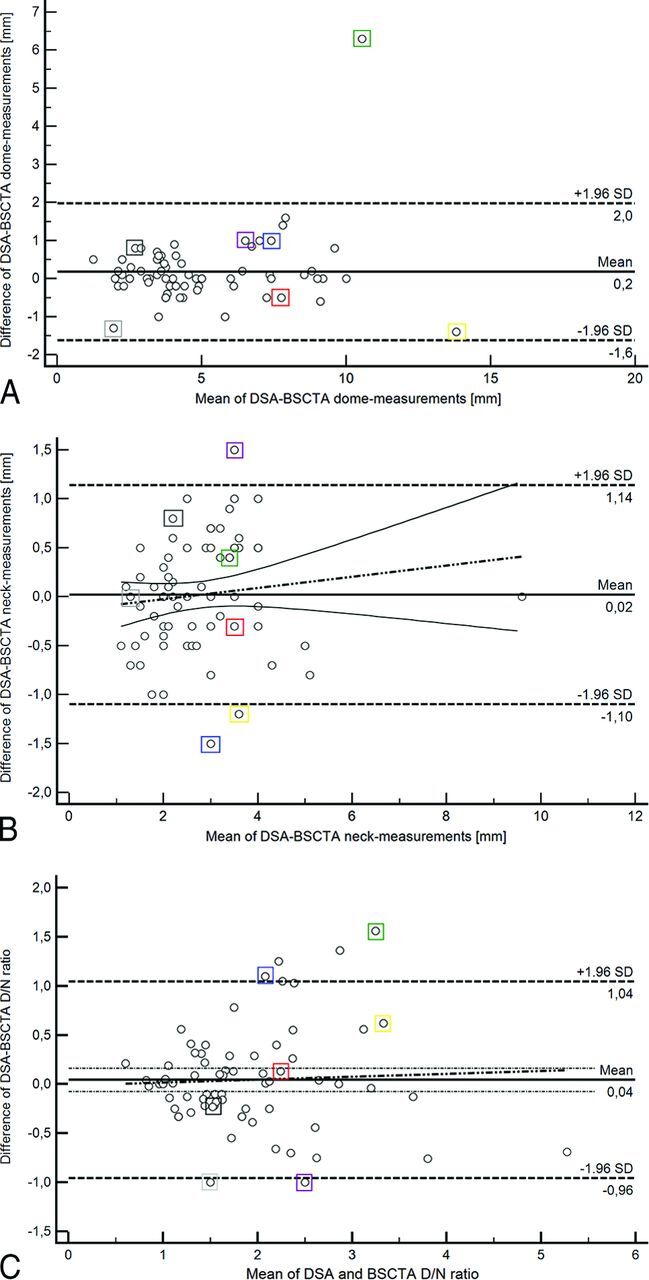
Results: Seventy-one patients (61%) had 74 aneurysms on DSA. Bone-subtraction CTA detected 73 of these aneurysms, but it detected 1 additional aneurysm. On a per-aneurysm basis, sensitivity, specificity, and positive and negative predictive values for bone-subtraction CTA were 99%, 98%, and 99% and 98%, respectively. For aneurysms of ≤3 mm, sensitivity was 94% (95% CI, 73%-99%). Bone-subtraction CTA slightly overestimated neck and dome diameters by <0.2 mm and overestimated the dome-to-neck ratios by 2% on average. Dose-length product was 565 ± 201 mGy × cm for bone-subtraction CTA and 1609 ± 1300 mGy × cm for DSA.
Conclusions: Bone-subtraction CTA is as accurate as DSA in detecting cerebral aneurysms after SAH, provides similar information about aneurysm configuration and measures, and reduces the average effective radiation dose for vascular diagnostics by 65%. Diagnostic equivalence in association with dose reduction suggests replacing DSA with bone-subtraction CTA in the diagnostic work-up of spontaneous SAH.
© 2016 by American Journal of Neuroradiology.
Figures
Similar articles
-
Dual-energy CT angiography in the evaluation of intracranial aneurysms: image quality, radiation dose, and comparison with 3D rotational digital subtraction angiography.AJR Am J Roentgenol. 2010 Jan;194(1):23-30. doi: 10.2214/AJR.08.2290. AJR Am J Roentgenol. 2010. PMID: 20028901
-
Comparison of the accuracy of subtraction CT angiography performed on 320-detector row volume CT with conventional CT angiography for diagnosis of intracranial aneurysms.Eur J Radiol. 2012 Jan;81(1):118-22. doi: 10.1016/j.ejrad.2011.05.003. Epub 2011 May 31. Eur J Radiol. 2012. PMID: 21632193
-
320-detector row CT angiography for detection and evaluation of intracranial aneurysms: comparison with conventional digital subtraction angiography.Clin Radiol. 2013 Jan;68(1):e15-20. doi: 10.1016/j.crad.2012.09.001. Epub 2012 Nov 9. Clin Radiol. 2013. PMID: 23142024
-
Comprehensive review of imaging of intracranial aneurysms and angiographically negative subarachnoid hemorrhage.Neurosurg Focus. 2019 Dec 1;47(6):E20. doi: 10.3171/2019.9.FOCUS19653. Neurosurg Focus. 2019. PMID: 31786554 Review.
-
Can computed tomography angiography of the brain replace lumbar puncture in the evaluation of acute-onset headache after a negative noncontrast cranial computed tomography scan?Acad Emerg Med. 2010 Apr;17(4):444-51. doi: 10.1111/j.1553-2712.2010.00694.x. Acad Emerg Med. 2010. PMID: 20370785 Review.
Cited by
-
Subtraction CT angiography in head and neck with low radiation and contrast dose dual-energy spectral CT using rapid kV-switching technique.Br J Radiol. 2018 Jun;91(1086):20170631. doi: 10.1259/bjr.20170631. Epub 2018 Mar 7. Br J Radiol. 2018. PMID: 29412008 Free PMC article.
-
Application of Spinal Subtraction and Bone Background Fusion CTA in the Accurate Diagnosis and Evaluation of Spinal Vascular Malformations.AJNR Am J Neuroradiol. 2024 Mar 7;45(3):351-357. doi: 10.3174/ajnr.A8112. AJNR Am J Neuroradiol. 2024. PMID: 38360787 Free PMC article.
-
Cerebral bone subtraction CT angiography using 80 kVp and sinogram-affirmed iterative reconstruction: contrast medium and radiation dose reduction with improvement of image quality.Neuroradiology. 2017 Feb;59(2):127-134. doi: 10.1007/s00234-016-1776-9. Epub 2017 Jan 3. Neuroradiology. 2017. PMID: 28050639
-
Metallic Component Preserving Algorithm Based on the Cerebral Computed Tomography Angiography in Aneurysm Surgery.Diagnostics (Basel). 2022 Jan 28;12(2):338. doi: 10.3390/diagnostics12020338. Diagnostics (Basel). 2022. PMID: 35204429 Free PMC article.
References
-
- Connolly ES Jr, Rabinstein AA, Carhuapoma JR, et al. ; American Heart Association Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular Nursing, Council on Cardiovascular Surgery and Anesthesia, Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012;43:1711–37 10.1161/STR.0b013e3182587839 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical