

Circulating nucleosomes as epigenetic biomarkers in pancreatic cancer
- PMID: 26451166
- PMCID: PMC4597435
- DOI: 10.1186/s13148-015-0139-4
Circulating nucleosomes as epigenetic biomarkers in pancreatic cancer
Abstract
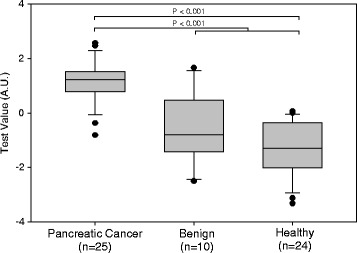
Background: To improve the prognosis of patients with pancreatic cancer, new biomarkers are required for earlier, pre-symptomatic diagnosis. Epigenetic mutations take place at the earliest stages of tumorigenesis and therefore offer new approaches for detecting and diagnosing disease. Nucleosomes are the repeating subunits of DNA and histone proteins that constitute human chromatin. Because of their release into the circulation, intact nucleosome levels in serum or plasma can serve as diagnostic disease biomarkers, and elevated levels have been reported in various cancers. However, quantifying nucleosomes in the circulation for cancer detection has been challenging due to nonspecific elevation in sera of patients with benign diseases. Here, we report for the first time differential, disease-associated epigenetic profiles of intact cell-free nucleosomes (cfnucleosomes) containing specific DNA and histone modifications as well as histone variants circulating in the blood. The study comprised serum samples from 59 individuals, including 25 patients with resectable pancreatic cancer, 10 patients with benign pancreatic disease, and 24 healthy individuals using Nucleosomics(®), a novel ELISA method.
Results: Multivariate analysis defined a panel of five serum cfnucleosome biomarkers that gave an area under the curve (AUC) of 0.95 for the discrimination of pancreatic cancer from healthy controls, which was superior to the diagnostic performance of the common pancreatic tumor biomarker, carbohydrate antigen 19-9 (CA 19-9) with an AUC of 0.87. Combining CA 19-9 with a panel of four cfnucleosome biomarkers gave an AUC of 0.98 with an overall sensitivity of 92 % at 90 % specificity.
Conclusions: The present study suggests that global epigenetic profiling of cfnucleosomes in serum using a simple NuQ(®) immunoassay-based approach can provide novel diagnostic biomarkers in pancreatic cancer.
Keywords: DNA; Diagnosis; Epigenetics; NuQ® assays; Nucleosomes; Pancreatic cancer; Screening; Serum.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources
