

What Is Needed to Eradicate Lymphatic Filariasis? A Model-Based Assessment on the Impact of Scaling Up Mass Drug Administration Programs
- PMID: 26451729
- PMCID: PMC4599939
- DOI: 10.1371/journal.pntd.0004147
What Is Needed to Eradicate Lymphatic Filariasis? A Model-Based Assessment on the Impact of Scaling Up Mass Drug Administration Programs
Abstract
Background: Lymphatic filariasis (LF) is a neglected tropical disease for which more than a billion people in 73 countries are thought to be at-risk. At a global level, the efforts against LF are designed as an elimination program. However, current efforts appear to aim for elimination in some but not all endemic areas. With the 2020 goal of elimination looming, we set out to develop plausible scale-up scenarios to reach global elimination and eradication. We predict the duration of mass drug administration (MDA) necessary to reach local elimination for a variety of transmission archetypes using an existing model of LF transmission, estimate the number of treatments required for each scenario, and consider implications of rapid scale-up.
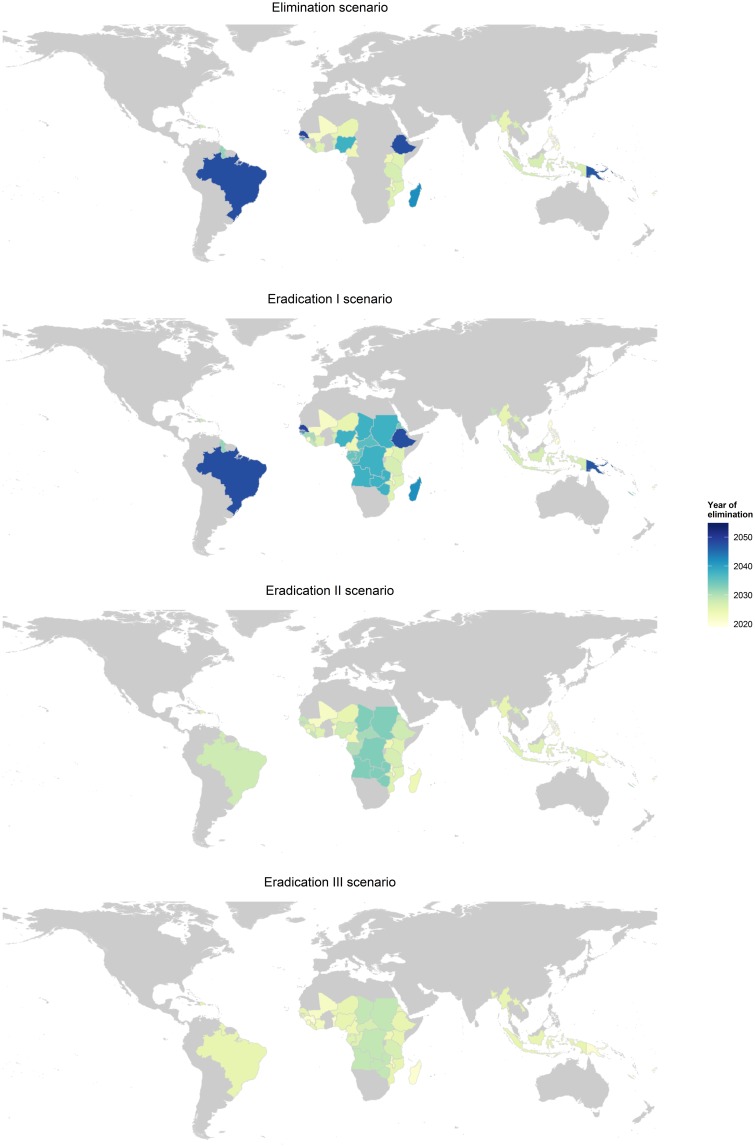
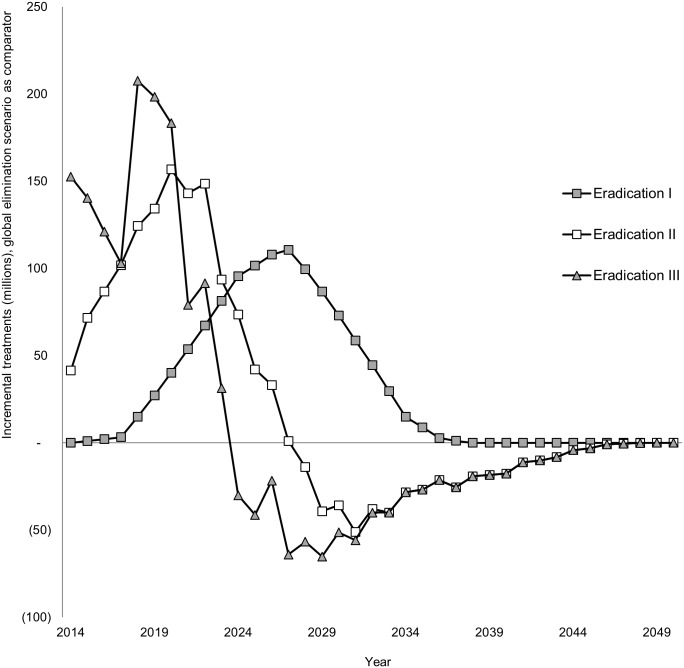
Methodology: We have defined four scenarios that differ in their geographic coverage and rate of scale-up. For each scenario, country-specific simulations and calculations were performed that took into account the pre-intervention transmission intensity, the different vector genera, drug regimen, achieved level of population coverage, previous progress toward elimination, and potential programmatic delays due to mapping, operations, and administration.
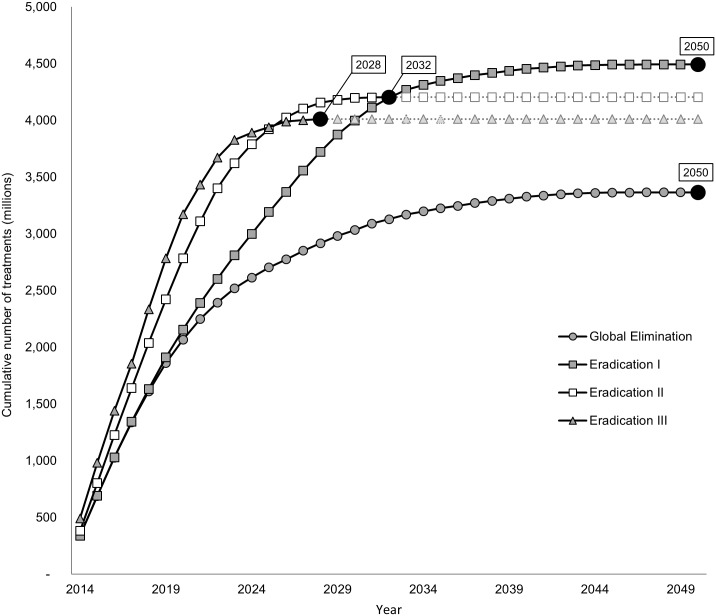
Principal findings: Our results indicate that eliminating LF by 2020 is unlikely. If MDA programs are drastically scaled up and expanded, the final round of MDA for LF eradication could be delivered in 2028 after 4,159 million treatments. However, if the current rate of scale-up is maintained, the final round of MDA to eradicate LF may not occur until 2050.
Conclusions/significance: Rapid scale-up of MDA will decrease the amount of time and treatments required to reach LF eradication. It may also propel the program towards success, as the risk of failure is likely to increase with extended program duration.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
How much will it cost to eradicate lymphatic filariasis? An analysis of the financial and economic costs of intensified efforts against lymphatic filariasis.PLoS Negl Trop Dis. 2017 Sep 26;11(9):e0005934. doi: 10.1371/journal.pntd.0005934. eCollection 2017 Sep. PLoS Negl Trop Dis. 2017. PMID: 28949987 Free PMC article.
-
Improving Coverage and Compliance in Mass Drug Administration for the Elimination of LF in Two 'Endgame' Districts in Indonesia Using Micronarrative Surveys.PLoS Negl Trop Dis. 2016 Nov 3;10(11):e0005027. doi: 10.1371/journal.pntd.0005027. eCollection 2016 Nov. PLoS Negl Trop Dis. 2016. PMID: 27812107 Free PMC article.
-
Assessing progress in reducing the at-risk population after 13 years of the global programme to eliminate lymphatic filariasis.PLoS Negl Trop Dis. 2014 Nov 20;8(11):e3333. doi: 10.1371/journal.pntd.0003333. eCollection 2014 Nov. PLoS Negl Trop Dis. 2014. PMID: 25411843 Free PMC article.
-
Progress towards elimination of lymphatic filariasis in the Eastern Mediterranean Region.Int Health. 2020 Dec 22;13(Suppl 1):S28-S32. doi: 10.1093/inthealth/ihaa037. Int Health. 2020. PMID: 33349874 Free PMC article. Review.
-
Toward the elimination of lymphatic filariasis by 2020: treatment update and impact assessment for the endgame.Expert Rev Anti Infect Ther. 2013 Jul;11(7):723-31. doi: 10.1586/14787210.2013.811841. Expert Rev Anti Infect Ther. 2013. PMID: 23879610 Review.
Cited by
-
Modelling the health impact and cost-effectiveness of lymphatic filariasis eradication under varying levels of mass drug administration scale-up and geographic coverage.BMJ Glob Health. 2016 Apr 6;1(1):e000021. doi: 10.1136/bmjgh-2015-000021. eCollection 2016. BMJ Glob Health. 2016. PMID: 28588916 Free PMC article.
-
Defining a prevalence level to describe the elimination of Lymphatic Filariasis (LF) transmission and designing monitoring & evaluating (M&E) programmes post the cessation of mass drug administration (MDA).PLoS Negl Trop Dis. 2020 Oct 12;14(10):e0008644. doi: 10.1371/journal.pntd.0008644. eCollection 2020 Oct. PLoS Negl Trop Dis. 2020. PMID: 33044958 Free PMC article.
-
The roadmap towards elimination of lymphatic filariasis by 2030: insights from quantitative and mathematical modelling.Gates Open Res. 2019 Sep 13;3:1538. doi: 10.12688/gatesopenres.13065.1. eCollection 2019. Gates Open Res. 2019. PMID: 31728440 Free PMC article.
-
Progress towards lymphatic filariasis elimination in Ghana from 2000-2016: Analysis of microfilaria prevalence data from 430 communities.PLoS Negl Trop Dis. 2019 Aug 9;13(8):e0007115. doi: 10.1371/journal.pntd.0007115. eCollection 2019 Aug. PLoS Negl Trop Dis. 2019. PMID: 31398203 Free PMC article.
-
Between-Country Inequalities in the Neglected Tropical Disease Burden in 1990 and 2010, with Projections for 2020.PLoS Negl Trop Dis. 2016 May 12;10(5):e0004560. doi: 10.1371/journal.pntd.0004560. eCollection 2016 May. PLoS Negl Trop Dis. 2016. PMID: 27171193 Free PMC article.
References
-
- WHO. Global programme to eliminate lymphatic filariasis: progress report for 2012. Wkly Epidemiol Rec. 2013;88(37): 389–99. Epub 2013/10/01. - PubMed
-
- de Souza DK, Koudou B, Kelly-Hope LA, Wilson MD, Bockarie MJ, Boakye DA. Diversity and transmission competence in lymphatic filariasis vectors in West Africa, and the implications for accelerated elimination of Anopheles-transmitted filariasis. Parasit Vectors. 2012;5: 259 10.1186/1756-3305-5-259 - DOI - PMC - PubMed
-
- Addiss DG, Dimock KA, Eberhard ML, Lammie PJ. Clinical, parasitologic, and immunologic observations of patients with hydrocele and elephantiasis in an area with endemic lymphatic filariasis. J Infect Dis. 1995;171(3): 755–8. - PubMed
-
- Suma TK, Shenoy RK, Kumaraswami V. A qualitative study of the perceptions, practices and socio-psychological suffering related to chronic brugian filariasis in Kerala, southern India. Ann Trop Med Parasitol. 2003;97(8): 839–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
