

Early oral switch therapy in low-risk Staphylococcus aureus bloodstream infection (SABATO): study protocol for a randomized controlled trial
- PMID: 26452342
- PMCID: PMC4600306
- DOI: 10.1186/s13063-015-0973-x
Early oral switch therapy in low-risk Staphylococcus aureus bloodstream infection (SABATO): study protocol for a randomized controlled trial
Abstract
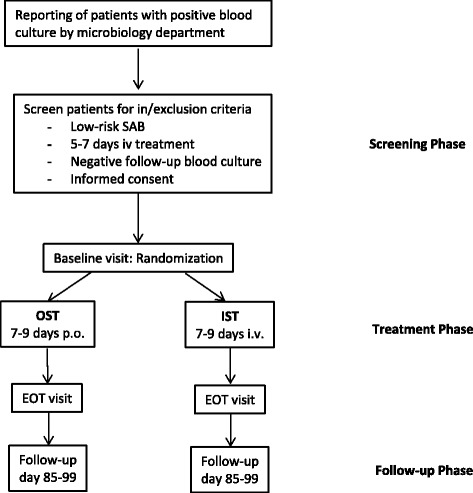
Background: Current guidelines recommend that patients with Staphylococcus aureus bloodstream infection (SAB) are treated with long courses of intravenous antimicrobial therapy. This serves to avoid SAB-related complications such as relapses, local extension and distant metastatic foci. However, in certain clinical scenarios, the incidence of SAB-related complications is low. Patients with a low-risk for complications may thus benefit from an early switch to oral medication through earlier discharge and fewer complications of intravenous therapy. The major objective for the SABATO trial is to demonstrate that in patients with low-risk SAB a switch from intravenous to oral antimicrobial therapy (oral switch therapy, OST) is non-inferior to a conventional course of intravenous therapy (intravenous standard therapy, IST).
Methods/design: The trial is designed as randomized, parallel-group, observer-blinded, clinical non-inferiority trial. The primary endpoint is the occurrence of a SAB-related complication (relapsing SAB, deep-seated infection, and attributable mortality) within 90 days. Secondary endpoints are the length of hospital stay; 14-day, 30-day, and 90-day mortality; and complications of intravenous therapy. Patients with SAB who have received 5 to 7 full days of adequate intravenous antimicrobial therapy are eligible. Main exclusion criteria are polymicrobial bloodstream infection, signs and symptoms of complicated SAB (deep-seated infection, hematogenous dissemination, septic shock, and prolonged bacteremia), the presence of a non-removable foreign body, and severe comorbidity. Patients will receive either OST or IST with a protocol-approved antimicrobial and are followed up for 90 days. Four hundred thirty patients will be randomized 1:1 in two study arms. Efficacy regarding incidence of SAB-related complications is tested sequentially with a non-inferiority margin of 10 and 5 percentage points.
Discussion: The SABATO trial assesses whether early oral switch therapy is safe and effective for patients with low-risk SAB. Regardless of the result, this pragmatic trial will strongly influence the standard of care in SAB.
Trial registration: ClinicalTrials.gov NCT01792804 registered 13 February 2013; German Clinical trials register DRKS00004741 registered 4 October 2013, EudraCT 2013-000577-77 . First patient randomized on 20 December 2013.

References
-
- WHO Global Strategy for Containment of Antimicrobial Resistance. World Health Organization;Geneva, 2001.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
