

Management and outcome of patients supported with Impella 5.0 for refractory cardiogenic shock
- PMID: 26453047
- PMCID: PMC4600310
- DOI: 10.1186/s13054-015-1073-8
Management and outcome of patients supported with Impella 5.0 for refractory cardiogenic shock
Abstract
Introduction: Cardiogenic shock refractory to standard therapy with inotropes and/or intra-aortic balloon pump is accompanied with an unacceptable high mortality. Percutaneous left ventricular assist devices may provide a survival benefit for these very sick patients. In this study, we describe our experience with the Impella 5.0 device used in the setting of refractory cardiogenic shock.
Methods: In this observational, retrospective, single-center study we included all the consecutive patients supported with Impella 5.0, between May 2008 and December 2013, for refractory cardiogenic shock. Patients' baseline and procedural characteristics, hemodynamics and outcome to the first 48 h of support, to ICU discharge and day-28 visit were collected.
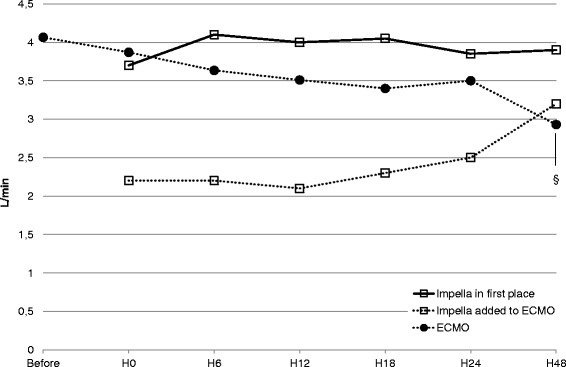
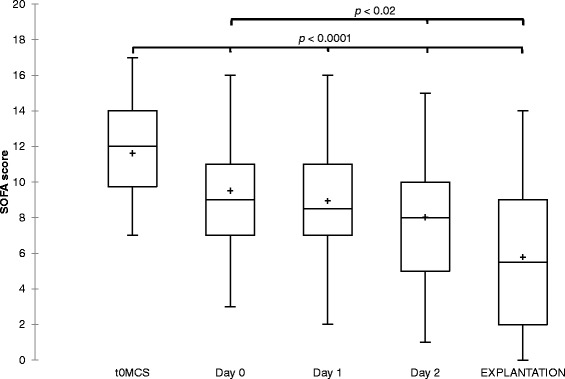
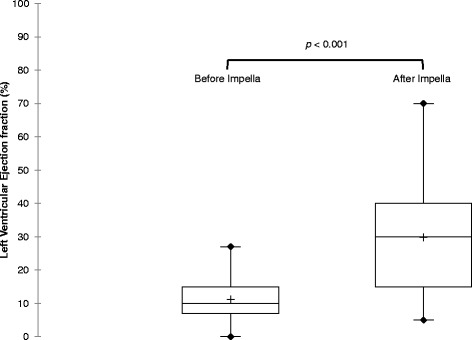
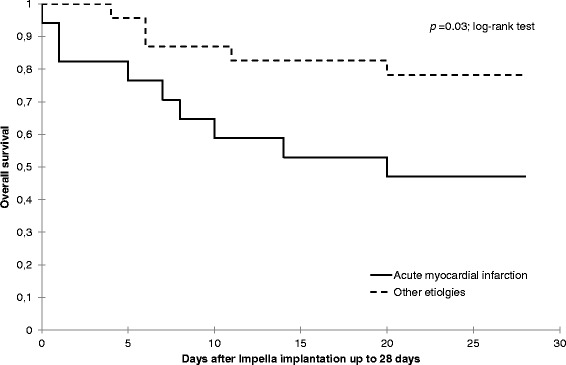
Results: A total of 40 patients were included in the study. Median age was 57 years and 87.5 % were male. Cardiogenic shock resulted from acute myocardial infarction in 17 patients (43 %), dilated cardiomyopathy in 12 (30 %) and postcardiotomy cardiac failure in 7 (18 %). In 15 patients Impella 5.0 was added to an ECMO to unload the left ventricle. The median SOFA score for the entire cohort prior to circulatory support was 12 [10-14] and the duration of Impella support was 7 [5-10] days. We observed a significant decrease of the inotrope score (10 [1-17] vs. 1 [0-9]; p = 0.04) and the lactate values (3.8 [1.7-5.9] mmol/L vs. 2.5 [1.5-3.4] mmol/L; p = 0.01) after 6 h of support with Impella 5.0. Furthermore, at Impella removal the patients' left ventricular ejection fraction improved significantly (p < 0.001) when compared to baseline. Cardiac recovery, bridge to left ventricular assist device or heart transplantation was possible in 28 patients (70 %). Twenty-six patients (65 %) survived at day 28. A multivariate analysis showed a higher risk of mortality for patients with acute myocardial infarction (hazard ratio = 4.1 (1.2-14.2); p = 0.02).
Conclusions: Impella 5.0 allowed fast weaning of inotropes and might facilitate myocardial recovery. Despite high severity scores at admission, day-28 mortality rate was better than predicated.
Figures
References
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–1847. doi: 10.1093/eurheartj/ehs104. - DOI - PubMed
-
- Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, et al. Intra-aortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock (IABP-SHOCK II): final 12 month results of a randomized, open-label trial. Lancet. 2013;382:1638–1645. doi: 10.1016/S0140-6736(13)61783-3. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
