

Postoperative Care Using a Secure Online Patient Portal: Changing the (Inter)Face of General Surgery
- PMID: 26453260
- PMCID: PMC4662904
- DOI: 10.1016/j.jamcollsurg.2015.08.429
Postoperative Care Using a Secure Online Patient Portal: Changing the (Inter)Face of General Surgery
Abstract
Background: Many patients seek greater accessibility to health care. Meanwhile, surgeons face increasing time constraints due to workforce shortages and elevated performance demands. Online postoperative care may improve patient access while increasing surgeon efficiency. We aimed to evaluate patient and surgeon acceptance of online postoperative care after elective general surgical operations.
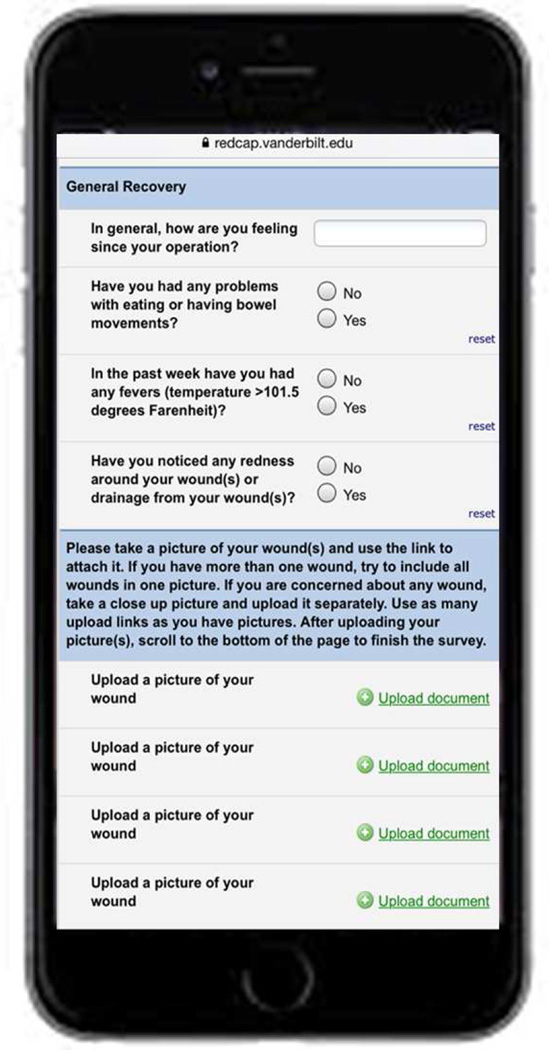
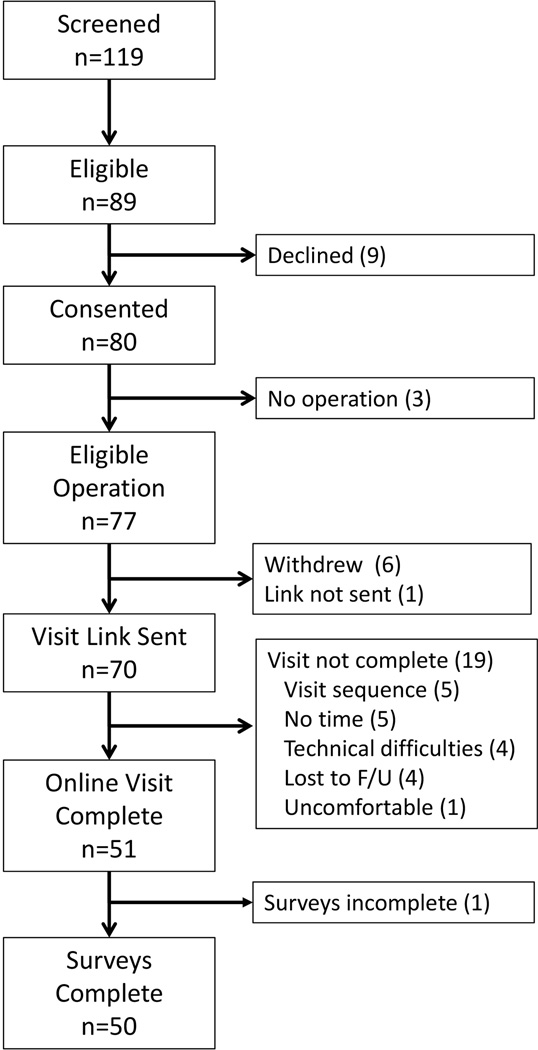
Study design: A prospective pilot study within an academic general surgery service compared online and in-person postoperative visits from May to December 2014. Included patients underwent elective laparoscopic cholecystectomy, laparoscopic ventral hernia repair, umbilical hernia repair, or inguinal hernia repair by 1 of 5 surgeons. Patients submitted symptom surveys and wound pictures, then corresponded with their surgeons using an online patient portal. The primary outcome was patient-reported acceptance of online visits in lieu of in-person visits. Secondary outcomes included detection of complications via online visits, surgeon-reported effectiveness, and visit times.
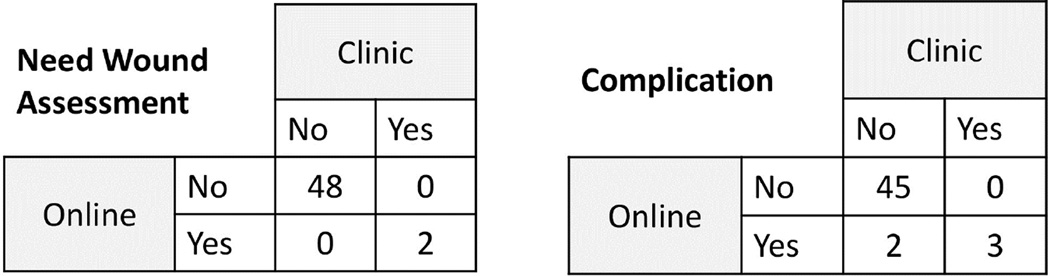
Results: Fifty patients completed both online and in-person visits. Online visits were acceptable to most patients as their only follow-up (76%). For 68% of patients, surgeons reported that both visit types were equally effective, while clinic visits were more effective in 24% and online visits in 8%. No complications were missed via online visits, which took significantly less time for patients (15 vs 103 minutes, p < 0.01) and surgeons (5 vs 10 minutes, p < 0.01).
Conclusions: In this population, online postoperative visits were accepted by patients and surgeons, took less time, and effectively identified patients who required further care. Further evaluation is needed to establish the safety and potential benefit of online postoperative visits in specific populations.
Published by Elsevier Inc.
Figures
Comment in
-
Re: Postoperative Care Using a Secure Online Patient Portal: Changing the (Inter)Face of General Surgery.J Urol. 2016 Aug;196(2):464-5. doi: 10.1016/j.juro.2016.03.170. Epub 2016 Apr 7. J Urol. 2016. PMID: 27479394 No abstract available.
References
-
- Porter M. The strategy that will fix healthcare. Harvard Bus Rev. 2013 Oct
-
- Detsky AS. What patients really want from health care. JAMA. 2011;306:2500–2501. - PubMed
-
- Institute of Medicine. Crossing the Quality Chasm. Washington, DC: National Academy Press; 2001.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
