

Recurrence Rate and Pattern of Perihilar Cholangiocarcinoma after Curative Intent Resection
- PMID: 26454735
- PMCID: PMC4736142
- DOI: 10.1016/j.jamcollsurg.2015.09.005
Recurrence Rate and Pattern of Perihilar Cholangiocarcinoma after Curative Intent Resection
Abstract
Background: The aim of this study was to investigate the rate and pattern of recurrence after curative intent resection of perihilar cholangiocarcinoma (PHC).
Study design: Patients were included from 2 prospectively maintained databases. Recurrences were categorized by site. Time to recurrence and recurrence-free survival (RFS) were estimated using the Kaplan-Meier method. Cox proportional hazards modeling was used to identify independent poor prognostic factors.
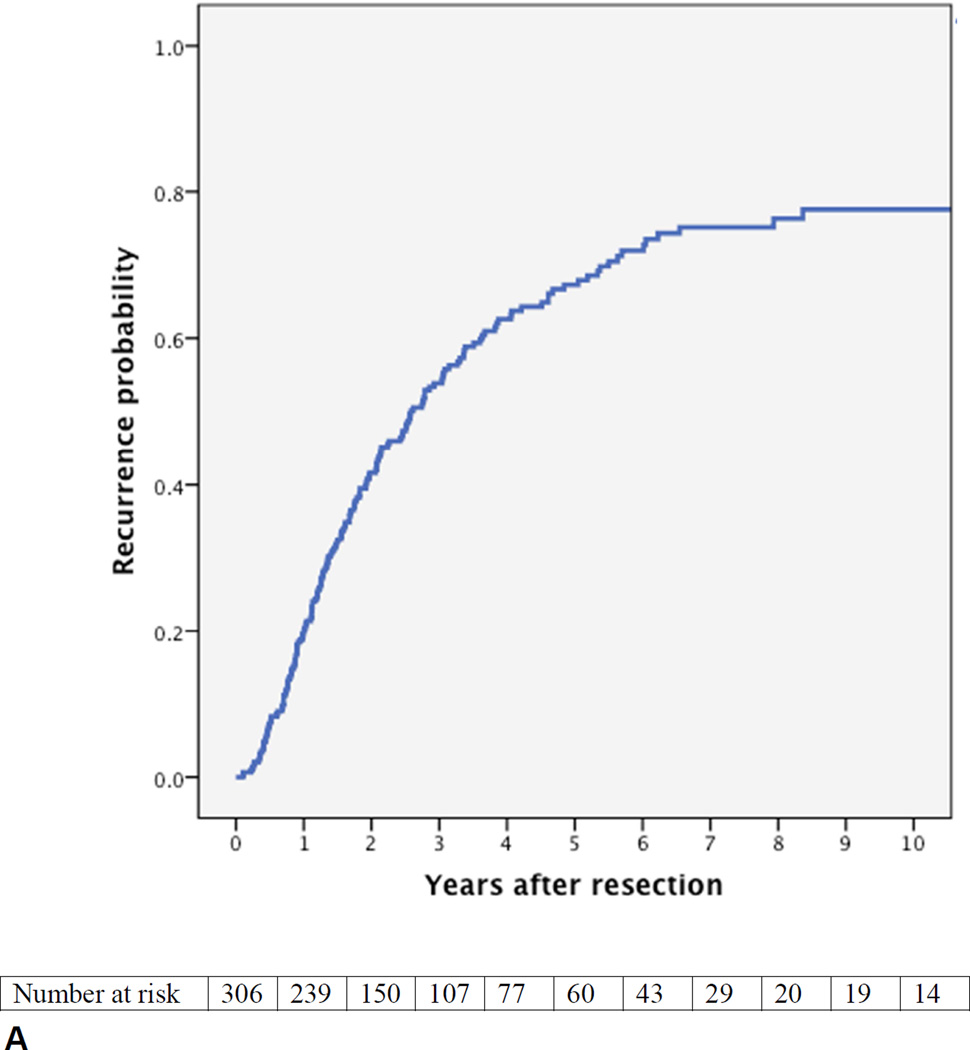
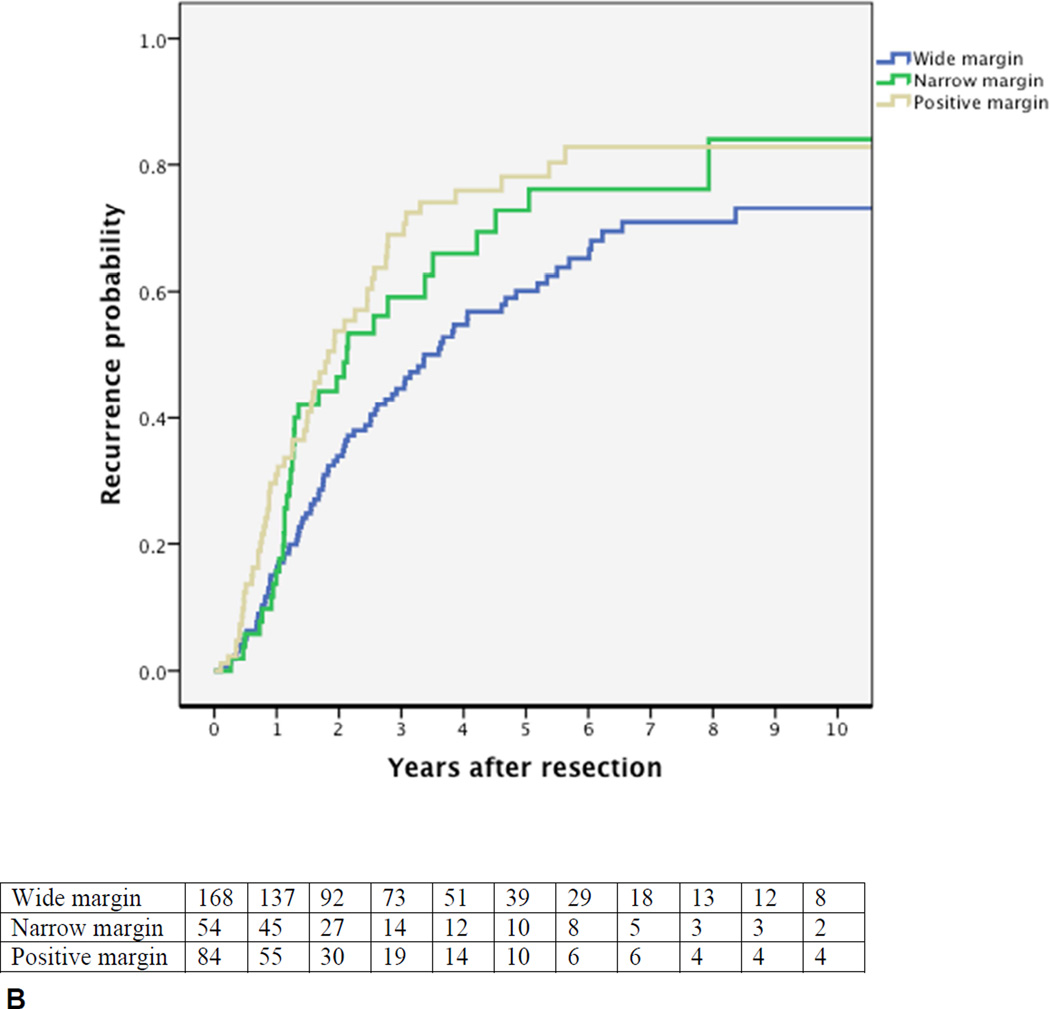
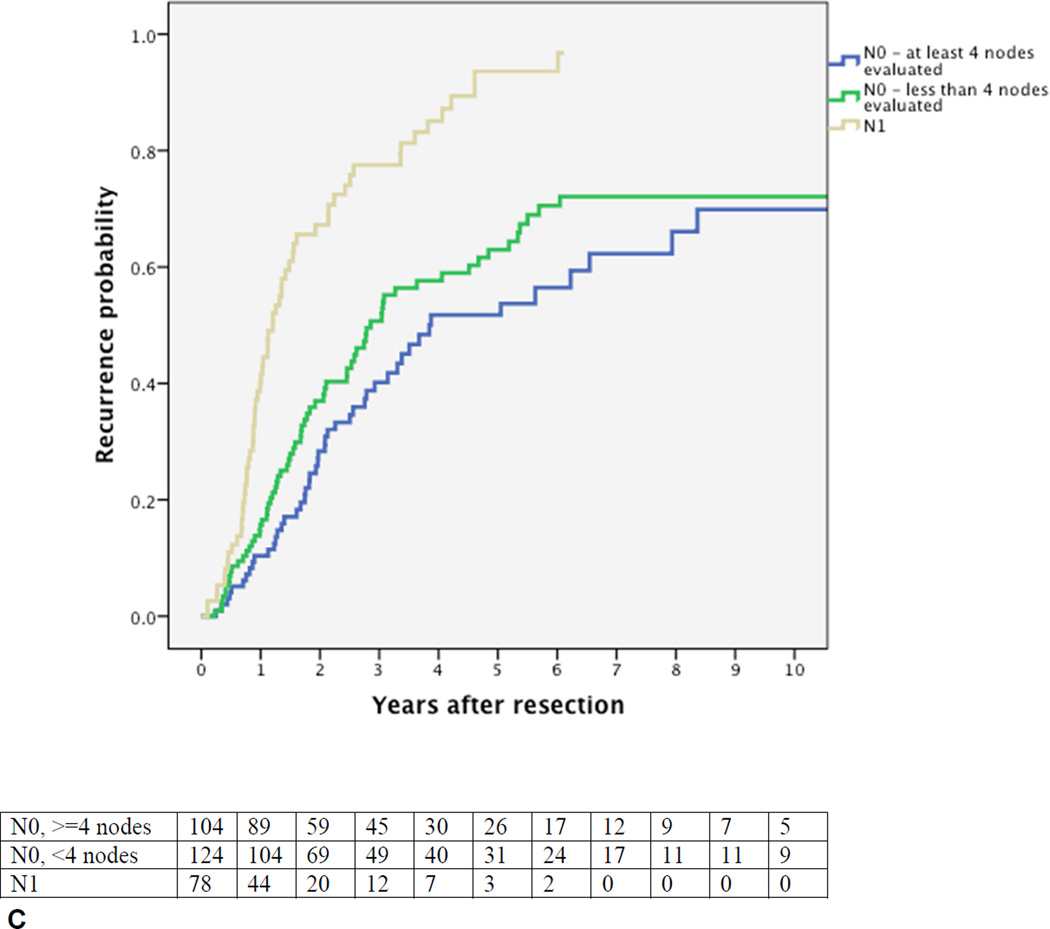
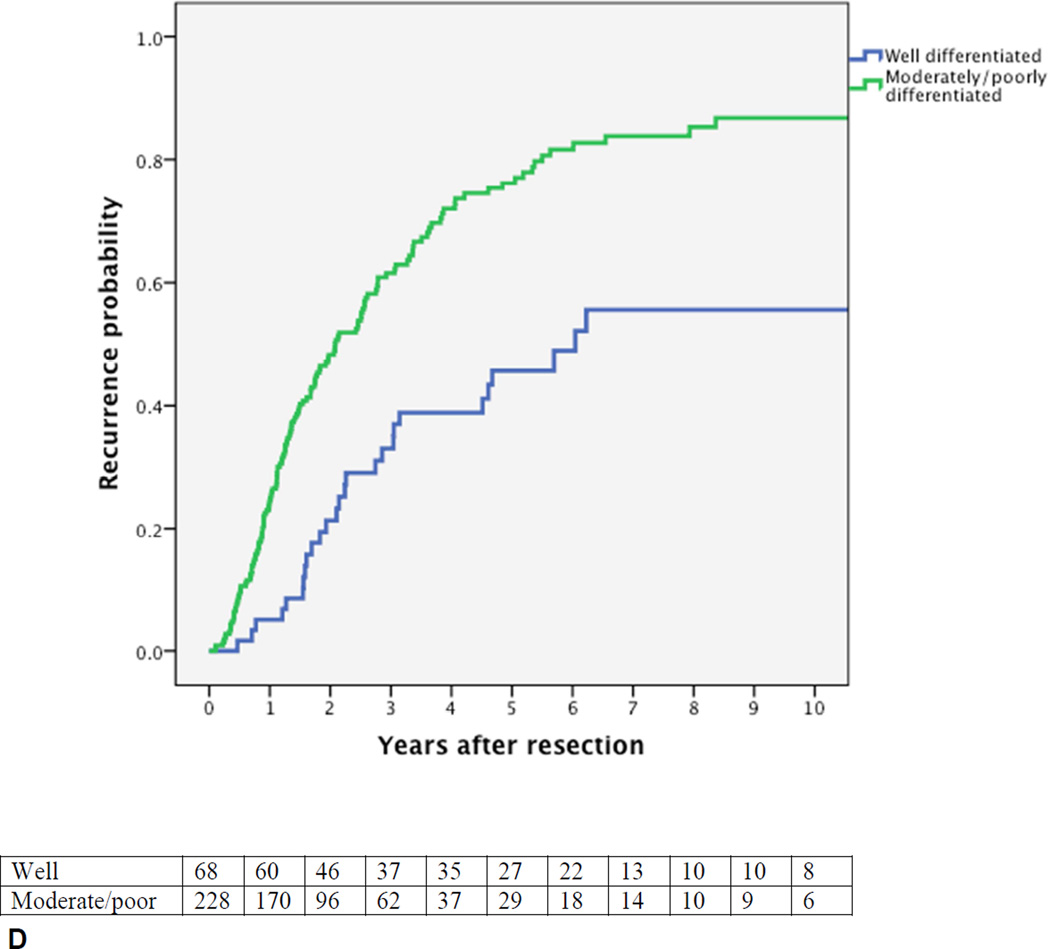
Results: Between 1991 and 2012, 306 consecutive patients met inclusion criteria. Median overall survival was 40 months. A recurrence was diagnosed in 177 patients (58%). An initial local recurrence was found in 26% of patients: liver hilum (11%), hepaticojejunostomy (8%), liver resection margin (8%), or distal bile duct remnant (2%). An initial distant recurrence was observed in 40% of patients: retroperitoneal lymph nodes (14%), intrahepatic away from the resection margin (13%), peritoneum (12%), and lungs (8%). Only 18% of patients had an isolated initial local recurrence. The estimated overall recurrence rate was 76% at 8 years. After a recurrence-free period of 5 years, 28% of patients developed a recurrence in the next 3 years. Median RFS was 26 months. Independent prognostic factors for RFS were resection margin, lymph node status, and tumor differentiation. Only node-positive PHC precluded RFS beyond 7 years.
Conclusions: Perihilar cholangiocarcinoma will recur in most patients (76%) after resection, emphasizing the need for better adjuvant strategies. The high recurrence rate of up to 8 years justifies prolonged surveillance. Only patients with an isolated initial local recurrence (18%) may have benefited from a more extensive resection or liver transplantation. Node-positive PHC appears incurable.
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Edge SB. AJCC Cancer Staging Manual. 7th. New York, USA: Springer; 2010.
-
- Popescu I, Dumitrascu T. Curative-intent surgery for hilar cholangiocarcinoma: prognostic factors for clinical decision making. Langenbeck's Arch Surg / Deutsche Gesellschaft fur Chirurgie. 2014;399:693–705. - PubMed
-
- Chen XP, Lau WY, Huang ZY, et al. Extent of liver resection for hilar cholangiocarcinoma. Br J Surg. 2009;96:1167–1175. - PubMed
-
- Dumitrascu T, Chirita D, Ionescu M, Popescu I. Resection for hilar cholangiocarcinoma: analysis of prognostic factors and the impact of systemic inflammation on long-term outcome. J Gastrointest Surg. 2013;17:913–924. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
