

Clinically Effective Treatment of Fibromyalgia Pain With High-Definition Transcranial Direct Current Stimulation: Phase II Open-Label Dose Optimization
- PMID: 26456677
- PMCID: PMC5777157
- DOI: 10.1016/j.jpain.2015.09.009
Clinically Effective Treatment of Fibromyalgia Pain With High-Definition Transcranial Direct Current Stimulation: Phase II Open-Label Dose Optimization
Abstract
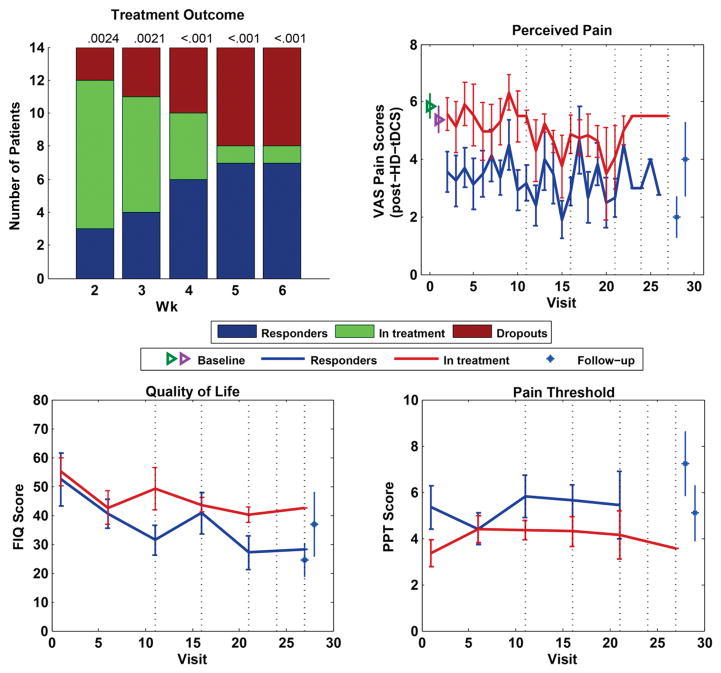
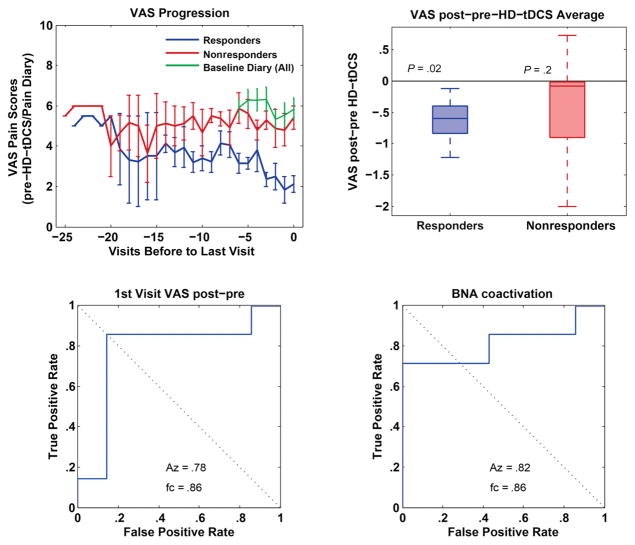
Despite promising preliminary results in treating fibromyalgia (FM) pain, no neuromodulation technique has been adopted in clinical practice because of limited efficacy, low response rate, or poor tolerability. This phase II open-label trial aims to define a methodology for a clinically effective treatment of pain in FM by establishing treatment protocols and screening procedures to maximize efficacy and response rate. High-definition transcranial direct current stimulation (HD-tDCS) provides targeted subthreshold brain stimulation, combining tolerability with specificity. We aimed to establish the number of HD-tDCS sessions required to achieve a 50% FM pain reduction, and to characterize the biometrics of the response, including brain network activation pain scores of contact heat-evoked potentials. We report a clinically significant benefit of a 50% pain reduction in half (n = 7) of the patients (N = 14), with responders and nonresponders alike benefiting from a cumulative effect of treatment, reflected in significant pain reduction (P = .035) as well as improved quality of life (P = .001) over time. We also report an aggregate 6-week response rate of 50% of patients and estimate 15 as the median number of HD-tDCS sessions to reach clinically meaningful outcomes. The methodology for a pivotal FM neuromodulation clinical trial with individualized treatment is thus supported.
Online registration: Registered in Clinicaltrials.gov under registry number NCT01842009.
Perspective: In this article, an optimized protocol for the treatment of fibromyalgia pain with targeted subthreshold brain stimulation using high-definition transcranial direct current stimulation is outlined.
Keywords: Fibromyalgia; high-definition transcranial direct current stimulation; motor cortex; noninvasive brain stimulation; pain.
Copyright © 2016 American Pain Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9:463–484. - PubMed
-
- Bannwarth B, Blotman F, Roue-Le Lay K, Caubere JP, Andre E, Taieb C. Fibromyalgia syndrome in the general population of France: a prevalence study. Joint Bone Spine. 2009;76:184–187. - PubMed
-
- Beck AT, Steer RA, Brown GK. BDI-II, Beck Depression Inventory: Manual. 2. San Antonio, TX.; Boston: Psychological Corp.; Harcourt Brace; 1996.
-
- Borckardt JJ, Bikson M, Frohman H, Reeves ST, Datta A, Bansal V, Madan A, Barth K, George MS. A pilot study of the tolerability and effects of high-definition transcranial direct current stimulation (HD-tDCS) on pain perception. J Pain. 2012;13:112–120. - PubMed
-
- Boyer L, Dousset A, Roussel P, Dossetto N, Cammilleri S, Piano V, Khalfa S, Mundler O, Donnet A, Guedj E. rTMS in fibromyalgia: a randomized trial evaluating QoL and its brain metabolic substrate. Neurology. 2014;82:1231–1238. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
