

SUDOSCAN: A Simple, Rapid, and Objective Method with Potential for Screening for Diabetic Peripheral Neuropathy
- PMID: 26457582
- PMCID: PMC4601729
- DOI: 10.1371/journal.pone.0138224
SUDOSCAN: A Simple, Rapid, and Objective Method with Potential for Screening for Diabetic Peripheral Neuropathy
Abstract
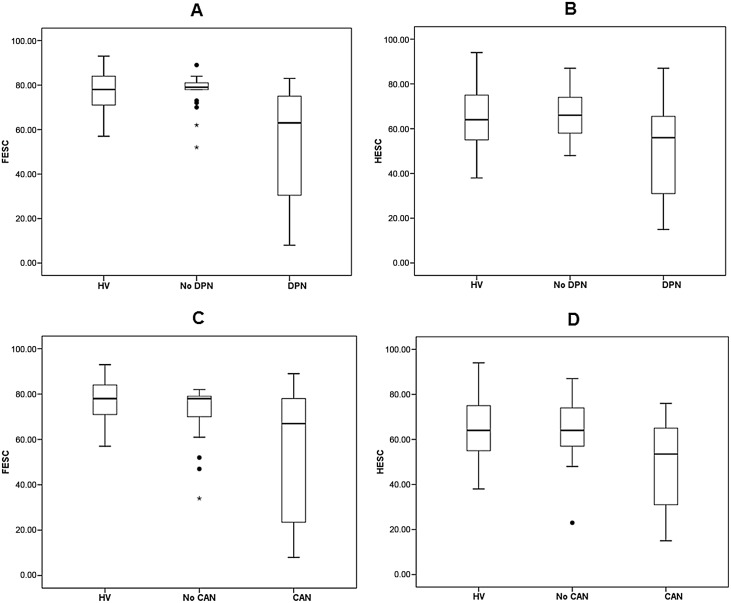
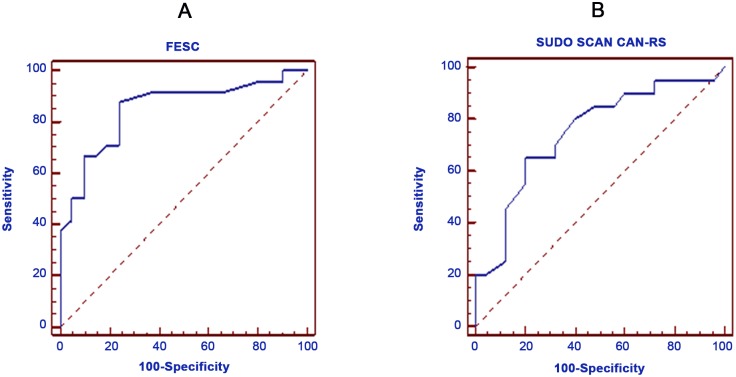
Clinical methods of detecting diabetic peripheral neuropathy (DPN) are not objective and reproducible. We therefore evaluated if SUDOSCAN, a new method developed to provide a quick, non-invasive and quantitative assessment of sudomotor function can reliably screen for DPN. 70 subjects (45 with type 1 diabetes and 25 healthy volunteers [HV]) underwent detailed assessments including clinical, neurophysiological and 5 standard cardiovascular reflex tests (CARTs). Using the American Academy of Neurology criteria subjects were classified into DPN and No-DPN groups. Based on CARTs subjects were also divided into CAN, subclinical-CAN and no-CAN. Sudomotor function was assessed with measurement of hand and foot Electrochemical Skin Conductance (ESC) and calculation of the CAN risk score. Foot ESC (μS) was significantly lower in subjects with DPN [n = 24; 53.5(25.1)] compared to the No-DPN [77.0(7.9)] and HV [77.1(14.3)] groups (ANCOVA p<0.001). Sensitivity and specificity of foot ESC for classifying DPN were 87.5% and 76.2%, respectively. The area under the ROC curve (AUC) was 0.85. Subjects with CAN had significantly lower foot [55.0(28.2)] and hand [53.5(19.6)] ESC compared to No-CAN [foot ESC, 72.1(12.2); hand ESC 64.9(14.4)] and HV groups (ANCOVA p<0.001 and 0.001, respectively). ROC analysis of CAN risk score to correctly classify CAN revealed a sensitivity of 65.0% and specificity of 80.0%. AUC was 0.75. Both foot and hand ESC demonstrated strong correlation with individual parameters and composite scores of nerve conduction and CAN. SUDOSCAN, a non-invasive and quick test, could be used as an objective screening test for DPN in busy diabetic clinics, insuring adherence to current recommendation of annual assessments for all diabetic patients that remains unfulfilled.
Conflict of interest statement
Figures

References
-
- Tesfaye S, Boulton AJM, Dyck PJ, Freeman R, Horowitz M, Kempler P et al. on behalf of The Toronto Diabetic Neuropathy Expert Group. Diabetic Neuropathies: Update on Definitions, Diagnostic Criteria, Estimation of Severity and Treatments. Diabetes Care 2010; 33: 2285–93. 10.2337/dc10-1303 - DOI - PMC - PubMed
-
- Boulton AJ, Kirsner RS, Vileik. Clinical practice. Neuropathic diabetic foot ulcers. N Engl J Med 2004. 351:48–55. - PubMed
-
- Forsblom CM, Sane T, Groop PH, Tötterman KJ, Kallio M, Saloranta C et al. Risk factors for mortality in Type II (non-insulin-dependent) diabetes: evidence of a role for neuropathy and a protective effect of HLA-DR4. Diabetologia 1998. 41:1253–62. - PubMed
-
- Hsu WC, Chiu SY, Yen AM, Chen LS, Fann CY, Liao CS et al. Somatic neuropathy is an independent predictor of all- and diabetes-related mortality in type 2 diabetic patients: a population-based 5-year follow-up study (KCIS No.29). Eur J Neurol 2012. 19:1192–8. 10.1111/j.1468-1331.2011.03659.x - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
