

Increasing Incidence of Extended-Spectrum β-Lactamase-Producing Escherichia coli in Community Hospitals throughout the Southeastern United States
- PMID: 26458226
- PMCID: PMC4748740
- DOI: 10.1017/ice.2015.239
Increasing Incidence of Extended-Spectrum β-Lactamase-Producing Escherichia coli in Community Hospitals throughout the Southeastern United States
Abstract
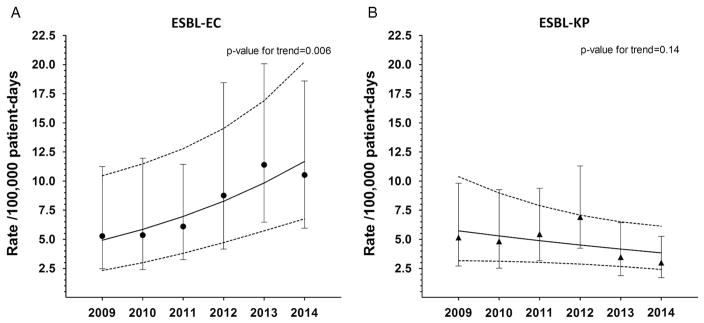
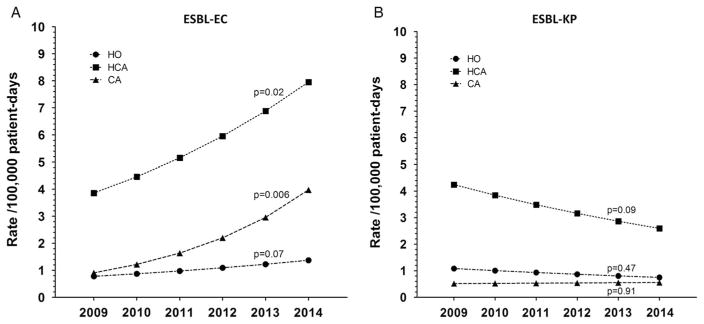
OBJECTIVE To describe the epidemiology of extended-spectrum β-lactamase (ESBL)-producing Escherichia coli (ESBL-EC) and Klebsiella pneumoniae (ESBL-KP) infections DESIGN Retrospective cohort SETTING Inpatient care at community hospitals PATIENTS All patients with ESBL-EC or ESBL-KP infections METHODS ESBL-EC and ESBL-KP infections from 26 community hospitals were prospectively entered into a centralized database from January 2009 to December 2014. RESULTS A total of 925 infections caused by ESBL-EC (10.5 infections per 100,000 patient days) and 463 infections caused by ESBL-KP (5.3 infections per 100,000 patient days) were identified during 8,791,243 patient days of surveillance. The incidence of ESBL-EC infections increased from 5.28 to 10.5 patients per 100,000 patient days during the study period (P=.006). The number of community hospitals with ESBL-EC infections increased from 17 (65%) in 2009 to 20 (77%) in 2014. The median ESBL-EC infection rates among individual hospitals with ≥1 ESBL-EC infection increased from 11.1 infections/100,000 patient days (range, 2.2-33.9 days) in 2009 to 22.1 infections per 100,000 patient days (range, 0.66-134 days) in 2014 (P=.05). The incidence of ESBL-KP infections remained constant over the study period (P=.14). Community-associated and healthcare-associated ESBL-EC infections trended upward (P=.006 and P=.02, respectively), while hospital-onset infections remained stable (P=.07). ESBL-EC infections were more common in females (54% vs 44%, P<.001) and Caucasians (50% vs 40%, P<.0001), and were more likely to be isolated from the urinary tract (61% vs 52%, P<.0001) than ESBL-KP infections. CONCLUSIONS The incidence of ESBL-EC infection has increased in community hospitals throughout the southeastern United States, while the incidence of ESBL-KP infection has remained stable. Community- and healthcare-associated ESBL-EC infections are driving the upward trend. Infect. Control Hosp. Epidemiol. 2015;37(1):49-54.
Conflict of interest statement
Figures
References
-
- Sidjabat HE, Paterson DL. Multidrug-resistant Escherichia coli in Asia: epidemiology and management. Expert Rev Anti Infect Ther. 2015:1–17. - PubMed
-
- Tansarli GS, Poulikakos P, Kapaskelis A, Falagas ME. Proportion of extended-spectrum beta-lactamase (ESBL)-producing isolates among Enterobacteriaceae in Africa: evaluation of the evidence—systematic review. J Antimicrob Chemother. 2014;69:1177–1184. - PubMed
-
- Coque TM, Baquero F, Canton R. Increasing prevalence of ESBL-producing Enterobacteriaceae in Europe. Euro Surveill. 2008;13:19044. - PubMed
-
- Bush K. Extended-spectrum beta-lactamases in North America, 1987–2006. Clin Microbiol Infect. 2008;14(Suppl 1):134–143. - PubMed
-
- Antimicrobial resistance surveillance in Europe. [Accessed June 18, 2015];European Centre for Disease Prevention and Control Web site. 2013 http://ecdc.europa.eu/en/publications/Publications/antimicrobial-resista.... Published 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
