

Evaluation of optimized breath-hold and free-breathing 3D ultrashort echo time contrast agent-free MRI of the human lung
- PMID: 26458867
- PMCID: PMC4833722
- DOI: 10.1002/jmri.25073
Evaluation of optimized breath-hold and free-breathing 3D ultrashort echo time contrast agent-free MRI of the human lung
Abstract
Purpose: To evaluate an optimized stack of radials ultrashort echo time (UTE) 3D magnetic resonance imaging (MRI) sequence for breath-hold and free-breathing imaging of the human lung.
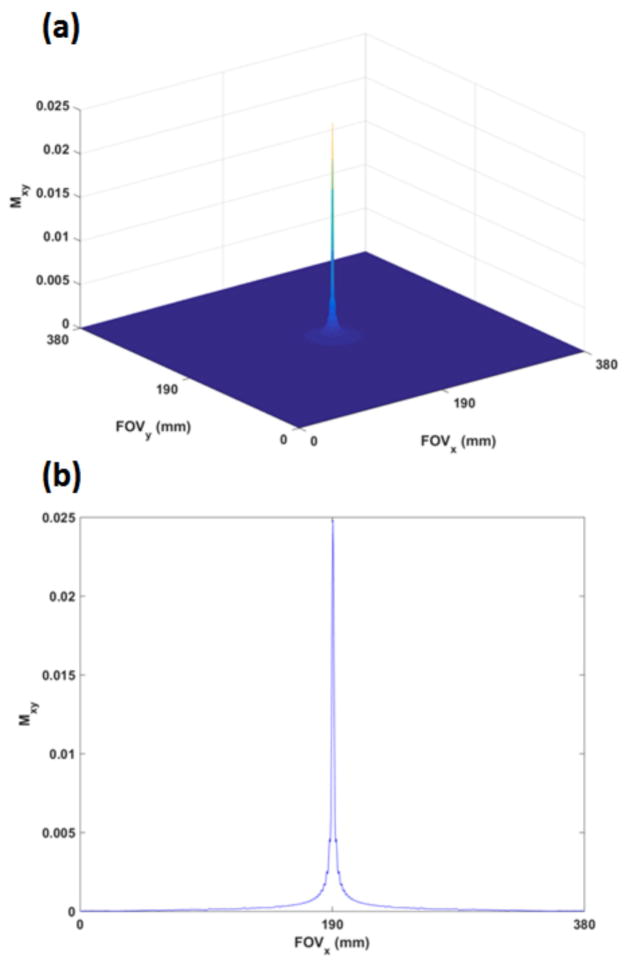
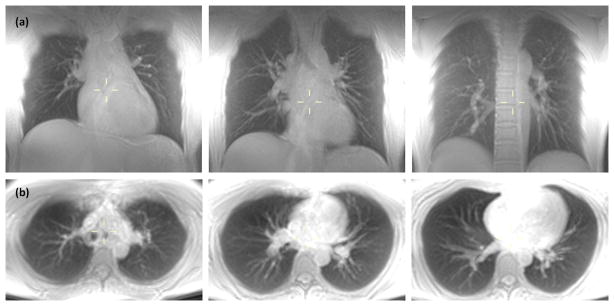
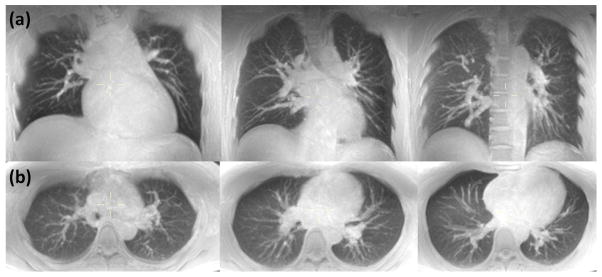
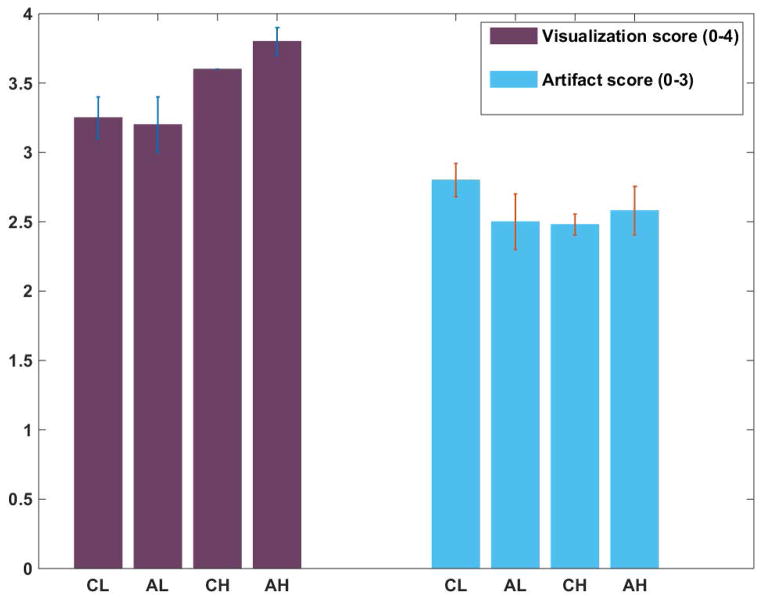
Materials and methods: A 3D stack of ultrashort echo time radials trajectory was optimized for coronal and axial lower-resolution breath-hold and higher-resolution free-breathing scans using Bloch simulations. The sequence was evaluated in 10 volunteers, without the use of contrast agents. Signal-to-noise ratio (SNR) mean and 95% confidence interval (CI) were determined from separate signal and noise images in a semiautomated fashion. The four scanning schemes were evaluated for significant differences in image quality using Student's t-test. Ten clinical patients were scanned with the sequence and findings were compared with concomitant computed tomography (CT) in nine patients. Breath-hold 3D spokes images were compared with 3D stack of radials in five volunteers. A Mann-Whitney U-test was performed to test significance in both cases.
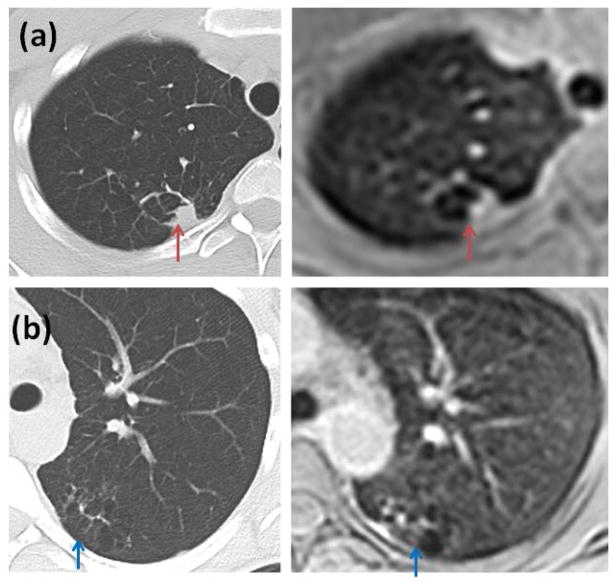
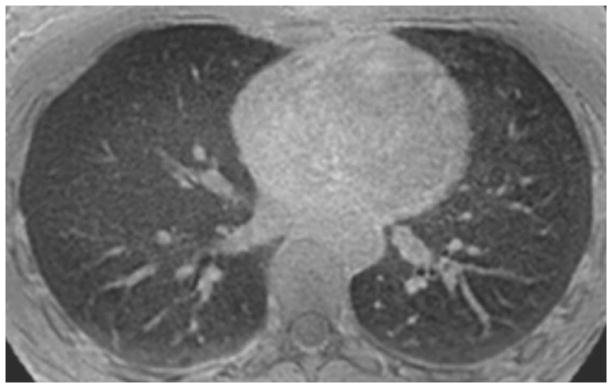
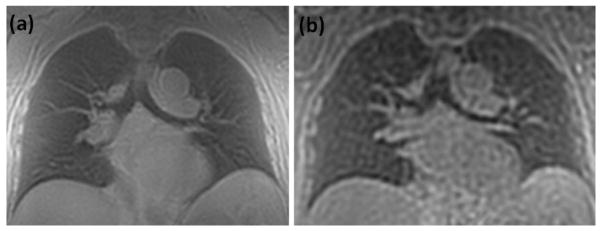
Results: Breath-hold imaging of the entire lung in volunteers was performed with SNR (mean = 42.5 [CI]: 35.5-49.5; mean = 34.3 [CI]: 28.6-40) in lung parenchyma for coronal and axial scans, respectively, which can be used as a quick scout scan. Longer respiratory triggered free-breathing scan enabled high-resolution UTE scanning with mean SNR of 14.2 ([CI]: 12.9-15.5) and 9.2 ([CI]: 8.2-10.2) for coronal and axial scans, respectively. Axial free-breathing scans showed significantly higher image quality (P = 0.008) than the three other scanning schemes. The mean score for comparison with CT was 1.67 (score 0: n = 0; 1: n = 3; 2: n = 6). There was no significant difference between CT and MRI (P = 0.25). 3D stack of radials images were significantly better than 3D spokes images (P < 0.001).
Conclusion: The optimized 3D stack of radials trajectory was shown to provide high-quality MR images of the lung parenchyma without the use of MRI contrast agents. The sequence may offer the possibility of breath-hold imaging and provides greater flexibility in trading off slice thickness and parallel imaging for scan time.
Keywords: 3D stack of radials; breath-hold; free-breathing; lung parenchyma.
© 2015 Wiley Periodicals, Inc.
Figures

References
-
- Kauczor HU, Ley-Zaporozhan J, Ley S. Imaging of pulmonary pathologies: focus on magnetic resonance imaging. Proc Am Thorac Soc. 2009;6(5):458–463. - PubMed
-
- Wielputz M, Kauczor HU. MRI of the lung: state of the art. Diagn Interv Radiol. 2012;18(4):344–353. - PubMed
-
- Zhang WJ, Hubbard Cristinacce PL, Bondesson E, et al. MR Quantitative Equilibrium Signal Mapping: A Reliable Alternative to CT in the Assessment of Emphysema in Patients with Chronic Obstructive Pulmonary Disease. Radiology. 2015;275(2):579–588. - PubMed
-
- Atkinson IC, Lu A, Thulborn KR. Characterization and correction of system delays and eddy currents for MR imaging with ultrashort echo-time and time-varying gradients. Magn Reson Med. 2009;62(2):532–537. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
