

Immunology of membranous nephropathy: from animal models to humans
- PMID: 26459770
- PMCID: PMC4711165
- DOI: 10.1111/cei.12729
Immunology of membranous nephropathy: from animal models to humans
Abstract
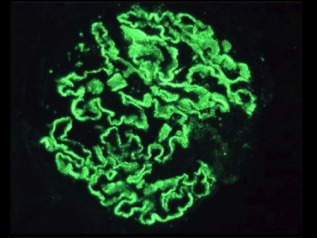
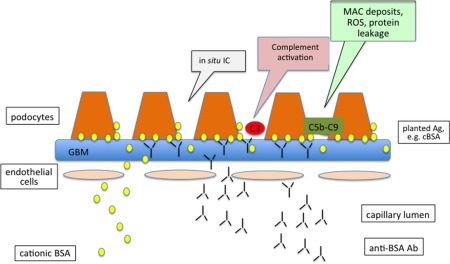
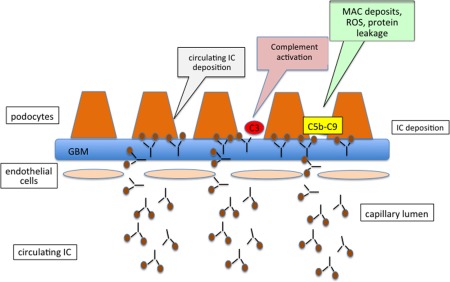
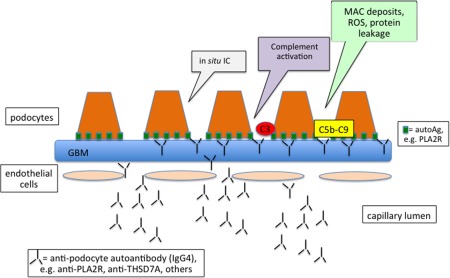
Membranous nephropathy (MN), the leading cause of nephrotic syndrome in adults, is characterized by the deposition of subepithelial immune deposits that consist mainly of immunoglobulin (Ig)G and complement. Most of the cases are primary or idiopathic (iMN), while only approximately 25% of the cases are secondary to some known disease such as systemic lupus erythematosus, hepatitis B, drugs and malignancies. Most of our knowledge on the pathogenesis of iMN has relied upon old experimental models (i.e. Heymann nephritis) that have shown that immune deposits are formed in situ by the reaction of autoantibodies against the respective podocyte antigen. Recent findings indicate that podocyte proteins also act as an autoantigen in human iMN. The M-type phospholipase A2 receptor (PLA2R) has been identified as the main target antigen, as it can be found in approximately 70% of iMN patients but only rarely in other glomerulonephritides. Podocytes damage in the experimental model of Heymann nephritis is complement-mediated. In humans, the presence of complement within the subepithelial deposits is well established, but IgG4, which does not activate complement by classical or alternative pathways, represents the predominant subclass of IgG anti-PLA2R. Some evidence suggests that IgG4 anti-PLA2R autoantibodies can bind mannan-binding lectin (MBL) and activate the lectin complement pathway. A genetic background for iMN has been demonstrated by genome-wide association studies that have shown highly significant associations of the PLA2R1 and the human leucocyte antigen (HLA)-DQA1 loci with iMN. In addition to their diagnostic value, anti-PLA2R antibodies may be useful to monitor disease activity and predict response to treatment.
Keywords: anti-PLA2R antibody; membranous nephropathy; podocyte; subepithelial deposits IgG4.
© 2015 British Society for Immunology.
Figures
References
-
- Tiebosch AT, Wolters J, Frederik PF, van der Wiel TW, Zeppenfeldt E, van Breda Vriesman PJ. Epidemiology of idiopathic glomerular disease: a prospective study. Kidney Int 1987; 32:112–6. - PubMed
-
- Maisonneuve P, Agodoa L, Gellert R et al Distribution of primary renal diseases leading to end‐stage renal failure in the United States, Europe, and Australia/New Zealand: results from an international comparative study. Am J Kidney Dis 2000; 35:157–65. - PubMed
-
- Mallick NP, Short CD, Manos J. Clinical membranous nephropathy. Nephron 1983; 34:209–19. - PubMed
-
- Jennette JC, Heptinstall RH. Heptinstall's pathology of the kidney. Philadelphia, PA: Lippincott Williams & Wilkins, 2007.
-
- Ehrenreich T, Churg J. Pathology of membranous nephropathy. In Pathology Annual 1968, New York, NY, Appleton‐Century‐Crofts, 1968; 3:145–86.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
