

Effect of patiromer on reducing serum potassium and preventing recurrent hyperkalaemia in patients with heart failure and chronic kidney disease on RAAS inhibitors
- PMID: 26459796
- PMCID: PMC5057342
- DOI: 10.1002/ejhf.402
Effect of patiromer on reducing serum potassium and preventing recurrent hyperkalaemia in patients with heart failure and chronic kidney disease on RAAS inhibitors
Abstract
Aims: We evaluated the effects of patiromer, a potassium (K(+))-binding polymer, in a pre-specified analysis of hyperkalaemic patients with heart failure (HF) in the OPAL-HK trial.
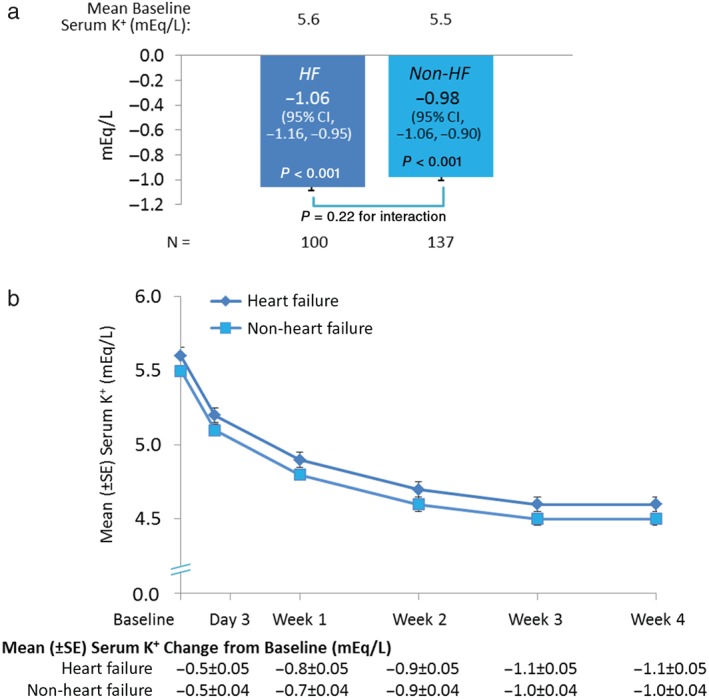
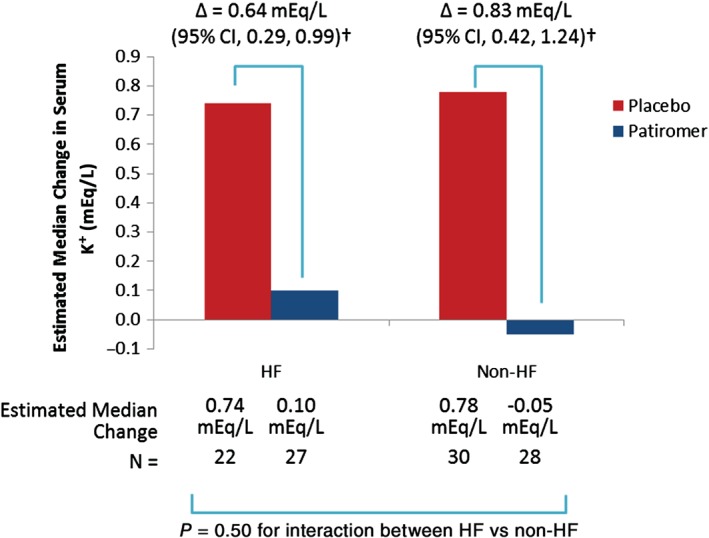
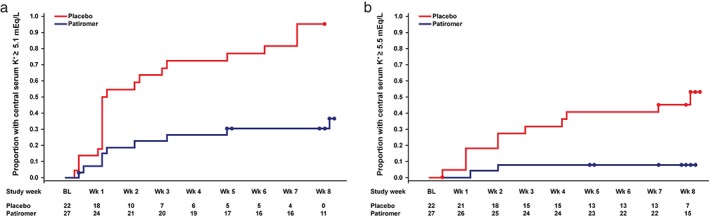
Methods and results: Chronic kidney disease (CKD) patients on renin-angiotensin-aldosterone system inhibitors (RAASi) with serum K(+) levels ≥5.1 mEq/L to <6.5 mEq/L (n = 243) received patiromer (4.2 g or 8.4 g BID initially) for 4 weeks (initial treatment phase); the primary efficacy endpoint was mean change in serum K(+) from baseline to week 4. Eligible patients (those with baseline K(+) ≥5.5 mEq/L to <6.5 mEq/L and levels ≥3.8 mEq/L to <5.1 mEq/L at the end of week 4) entered an 8-week randomized withdrawal phase and were randomly assigned to continue patiromer or switch to placebo; the primary efficacy endpoint was the between-group difference in median change in the serum K(+) over the first 4 weeks of that phase. One hundred and two patients (42%) had heart failure (HF). The mean [± standard error (SE)] change in serum K(+) from baseline to week 4 was -1.06 ± 0.05 mEq/L [95% confidence interval (CI), -1.16,-0.95; P < 0.001]; 76% (95% CI, 69,84) achieved serum K(+), 3.8 mEq/L to <5.1 mEq/L. In the randomized withdrawal phase, the median increase in serum K(+) from baseline of that phase was greater with placebo (n = 22) than patiromer (n = 27) (P < 0.001); recurrent hyperkalaemia (serum K(+), ≥5.5 mEq/L) occurred in 52% on placebo and 8% on patiromer (P < 0.001). Mild-to-moderate constipation was the most common adverse event (11%); hypokalaemia occurred in 3%.
Conclusion: In patients with CKD and HF who were hyperkalaemic on RAASi, patiromer was well tolerated, decreased serum K(+), and, compared with placebo, reduced recurrent hyperkalaemia.
Keywords: chronic kidney disease; heart failure; hyperkalaemia; patiromer.
© 2015 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Comment in
-
Hyperkalaemia in heart failure: binding the patient to improved treatment?Eur J Heart Fail. 2015 Oct;17(10):997-9. doi: 10.1002/ejhf.404. Epub 2015 Oct 7. Eur J Heart Fail. 2015. PMID: 26443125 No abstract available.
-
Response to: Hyperkalaemia in heart failure: binding the patient to improved treatment?Eur J Heart Fail. 2016 Feb;18(2):216. doi: 10.1002/ejhf.452. Epub 2015 Dec 3. Eur J Heart Fail. 2016. PMID: 26634417 Free PMC article. No abstract available.
References
-
- Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, Palensky J, Wittes J. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999;341:709–717. - PubMed
-
- Zannad F, McMurray JJ, Krum H, van Veldhuisen, DJ , Swedberg K, Shi H, Vincent J, Pocock SJ, Pitt B. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 2011;364:11–21.
-
- Sorensen MV, Matos JE, Praetorius HA, Leipziger J. Colonic potassium handling. Pflugers Arch 2010;459:645–656. - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez‐Sanchez MA, Jaarsma T, Køber L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rønnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14:803–869. - PubMed
-
- Kidney Disease Outcomes Quality Initiative (K/DOQI) . K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis 2004;43:S1–S290. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
