

Risk Factors For Stroke, Myocardial Infarction, or Death Following Carotid Endarterectomy: Results From the International Carotid Stenting Study
- PMID: 26460291
- PMCID: PMC4684145
- DOI: 10.1016/j.ejvs.2015.08.006
Risk Factors For Stroke, Myocardial Infarction, or Death Following Carotid Endarterectomy: Results From the International Carotid Stenting Study
Abstract
Objectives: Carotid endarterectomy (CEA) is standard treatment for symptomatic carotid artery stenosis but carries a risk of stroke, myocardial infarction (MI), or death. This study investigated risk factors for these procedural complications occurring within 30 days of endarterectomy in the International Carotid Stenting Study (ICSS).
Methods: Patients with recently symptomatic carotid stenosis >50% were randomly allocated to endarterectomy or stenting. Analysis is reported of patients in ICSS assigned to endarterectomy and limited to those in whom CEA was initiated. The occurrence of stroke, MI, or death within 30 days of the procedure was reported by investigators and adjudicated. Demographic and technical risk factors for these complications were analysed sequentially in a binomial regression analysis and subsequently in a multivariable model.
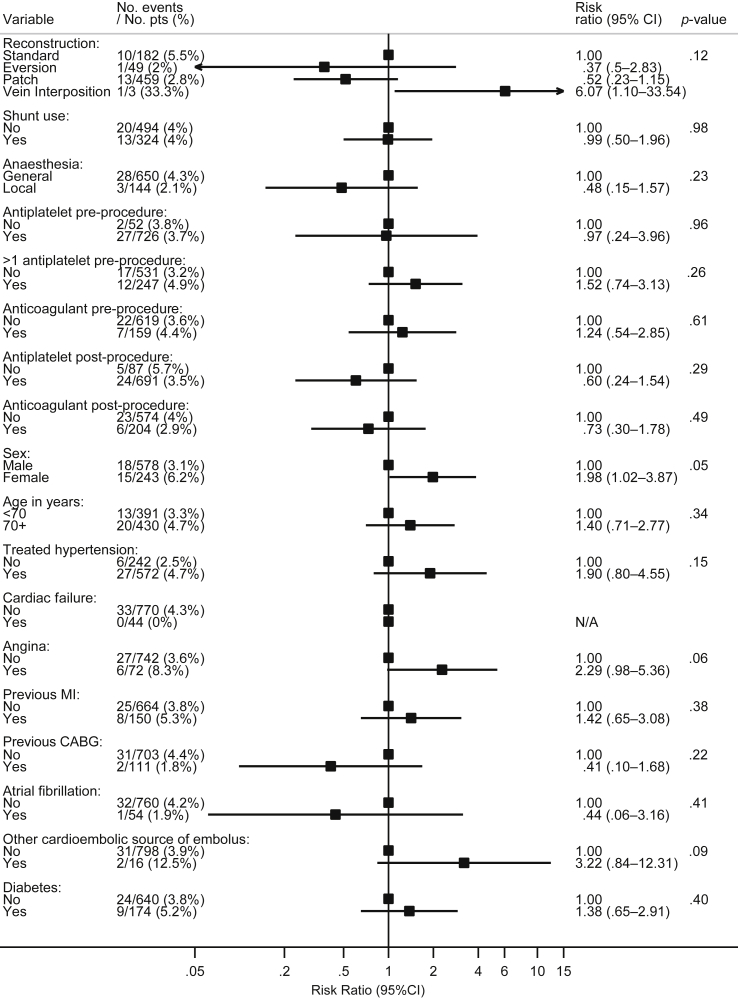
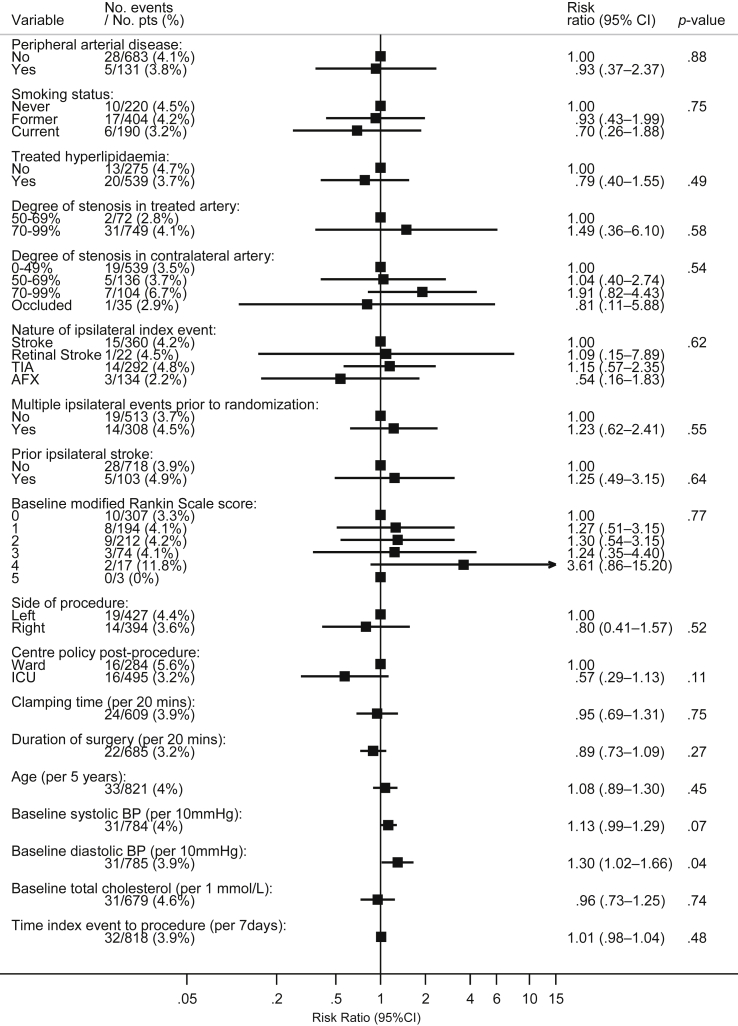
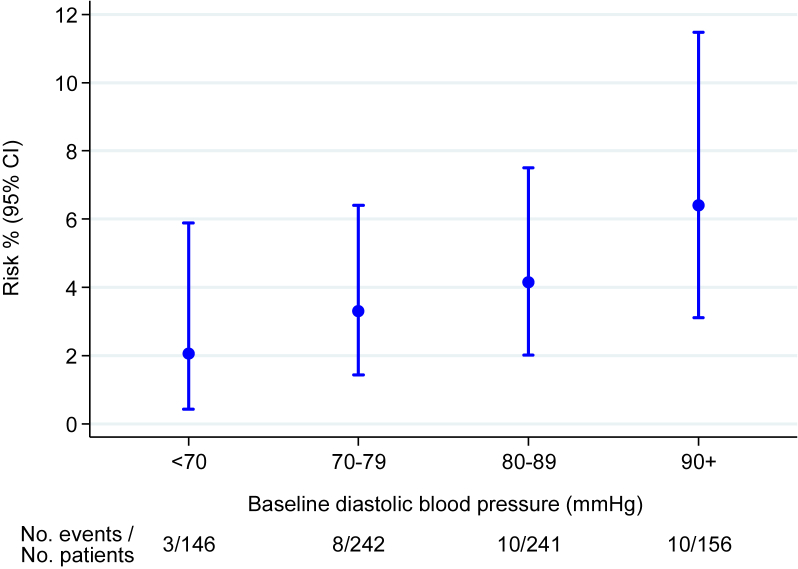
Results: Eight-hundred and twenty-one patients were included in the analysis. The risk of stroke, MI, or death within 30 days of CEA was 4.0%. The risk was higher in female patients (risk ratio [RR] 1.98, 95% CI 1.02-3.87, p = .05) and with increasing baseline diastolic blood pressure (dBP) (RR 1.30 per +10 mmHg, 95% CI 1.02-1.66, p = .04). Mean baseline dBP, obtained at the time of randomization in the trial, was 78 mmHg (SD 13 mmHg). In a multivariable model, only dBP remained a significant predictor. The risk was not related to the type of surgical reconstruction, anaesthetic technique, or perioperative medication regimen. Patients undergoing CEA stayed a median of 4 days before discharge, and 21.2% of events occurred on or after the day of discharge.
Conclusions: Increasing diastolic blood pressure was the only independent risk factor for stroke, MI, or death following CEA. Cautious attention to blood pressure control following symptoms attributable to carotid stenosis could reduce the risks associated with subsequent CEA.
Keywords: Carotid artery stenosis; Carotid atherosclerosis; Carotid endarterectomy.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Barnett H.J.M., Taylor D.W., Eliasziw M., Fox A.J., Ferguson G.G., Haynes R.B., for the North American Symptomatic Carotid Endarterectomy Trial Collaborators Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. New Engl J Med. 1998;339:1415–1425. - PubMed
-
- Farrell B., Fraser A., Sandercock P., Slattery J., Warlow C.P. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998;351:1379–1387. - PubMed
-
- Mayberg M.R., Wilson S.E., Yatsu F., Weiss D.G., Messina L., Hershey L.A. Carotid endarterectomy and prevention of cerebral ischaemia in symptomatic carotid stenosis. JAMA. 1991;226:3289–3294. - PubMed
-
- Rerkasem K., Rothwell P.M. Carotid endarterectomy for symptomatic carotid stenosis. Cochrane Database Syst Rev. 2011;(4) Art. No.: CD001081. http://dx.doi.org/10.1002/14651858.CD001081.pub2. - DOI - PubMed
-
- Rothwell P.M., Rerkasem K. Temporal trends in the risks of stroke and death due to endarterectomy for symptomatic carotid stenosis: an updated systematic review. Eur J Vasc Endovasc. 2009;37:504–511. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
