

Phase II Pilot Study of Vemurafenib in Patients With Metastatic BRAF-Mutated Colorectal Cancer
- PMID: 26460303
- PMCID: PMC4669589
- DOI: 10.1200/JCO.2015.63.2497
Phase II Pilot Study of Vemurafenib in Patients With Metastatic BRAF-Mutated Colorectal Cancer
Abstract
Purpose: BRAF V600E mutation is seen in 5% to 8% of patients with metastatic colorectal cancer (CRC) and is associated with poor prognosis. Vemurafenib, an oral BRAF V600 inhibitor, has pronounced activity in patients with metastatic melanoma, but its activity in patients with BRAF V600E-positive metastatic CRC was unknown.
Patients and methods: In this multi-institutional, open-label study, patients with metastatic CRC with BRAF V600 mutations were recruited to an expansion cohort at the previously determined maximum-tolerated dose of 960 mg orally twice a day.
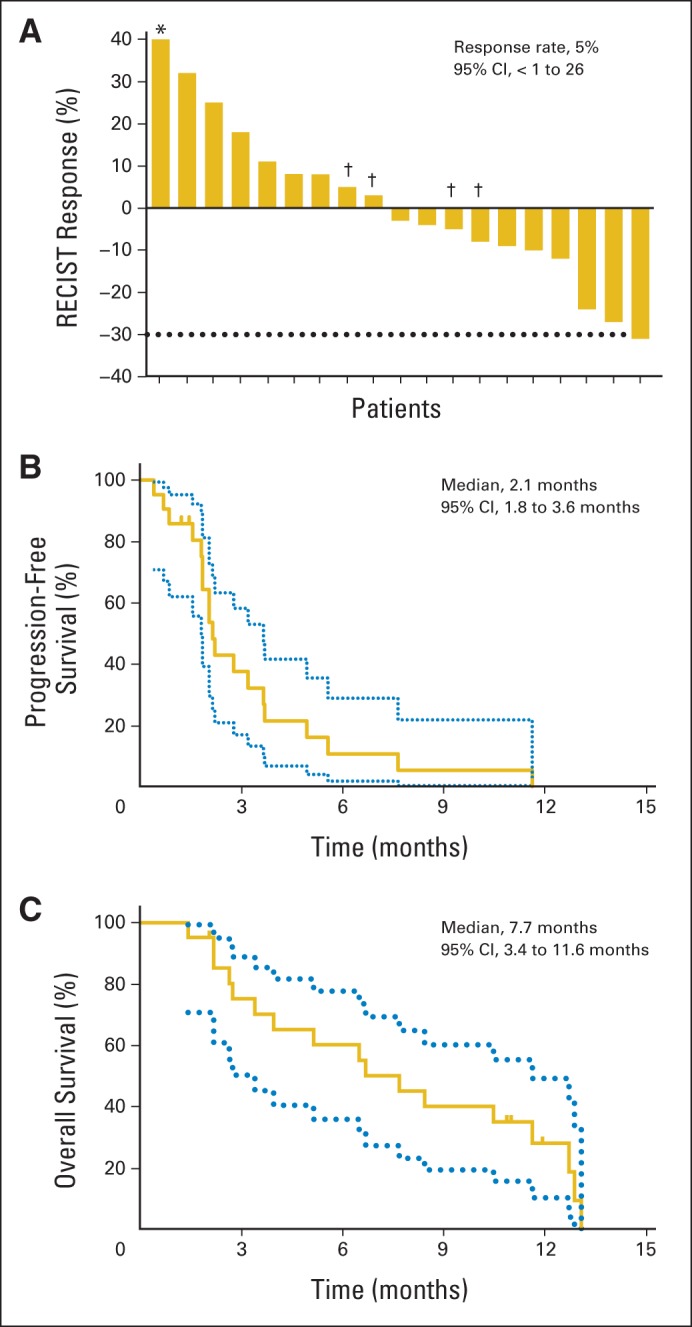
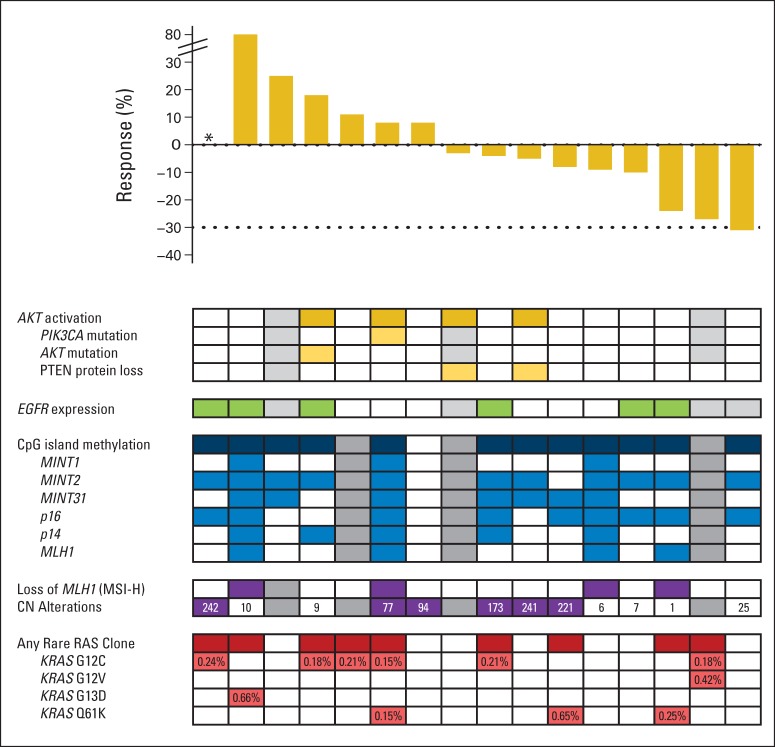
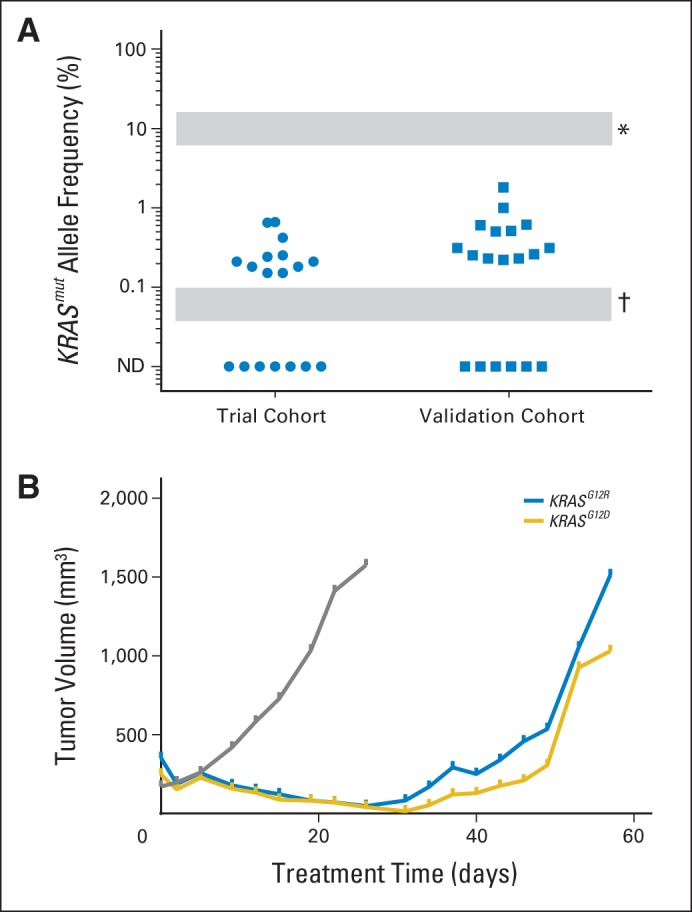
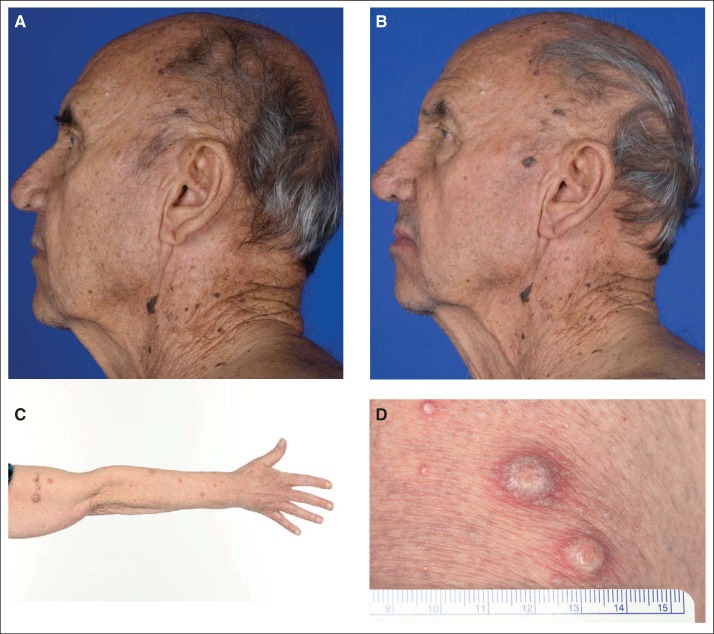
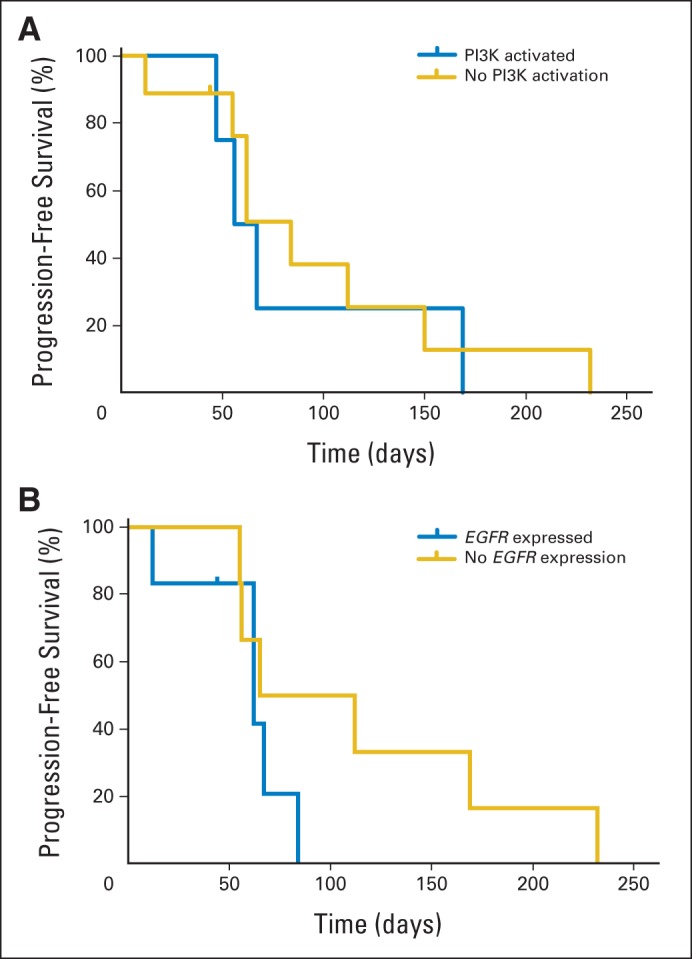
Results: Twenty-one patients were enrolled, of whom 20 had received at least one prior metastatic chemotherapy regimen. Grade 3 toxicities included keratoacanthomas, rash, fatigue, and arthralgia. Of the 21 patients treated, one patient had a confirmed partial response (5%; 95% CI, 1% to 24%) and seven other patients had stable disease by RECIST criteria. Median progression-free survival was 2.1 months. Patterns of concurrent mutations, microsatellite instability status, CpG island methylation status, PTEN loss, EGFR expression, and copy number alterations were not associated with clinical benefit. In contrast to prior expectations, concurrent KRAS and NRAS mutations were detected at low allele frequency in a subset of the patients' tumors (median, 0.21% allele frequency) and were apparent mechanisms of acquired resistance in vemurafenib-sensitive patient-derived xenograft models.
Conclusion: In marked contrast to the results seen in patients with BRAF V600E-mutant melanoma, single-agent vemurafenib did not show meaningful clinical activity in patients with BRAF V600E mutant CRC. Combination strategies are now under development and may be informed by the presence of intratumor heterogeneity of KRAS and NRAS mutations.
Trial registration: ClinicalTrials.gov NCT00405587.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Hitting the Target in BRAF-Mutant Colorectal Cancer.J Clin Oncol. 2015 Dec 1;33(34):3990-2. doi: 10.1200/JCO.2015.63.7793. Epub 2015 Oct 12. J Clin Oncol. 2015. PMID: 26460302 No abstract available.
-
Colorectal cancer: Targeting BRAF mutations equally?Nat Rev Clin Oncol. 2016 Jan;13(1):4. doi: 10.1038/nrclinonc.2015.190. Epub 2015 Nov 10. Nat Rev Clin Oncol. 2016. PMID: 26552951 No abstract available.
References
-
- Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–954. - PubMed
-
- Michaloglou C, Vredeveld LC, Mooi WJ, et al. BRAF(E600) in benign and malignant human tumours. Oncogene. 2008;27:877–895. - PubMed
-
- Joneson T, Bar-Sagi D. Ras effectors and their role in mitogenesis and oncogenesis. J Mol Med (Berl) 1997;75:587–593. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
