

Perforated peptic ulcer
- PMID: 26460663
- PMCID: PMC4618390
- DOI: 10.1016/S0140-6736(15)00276-7
Perforated peptic ulcer
Abstract
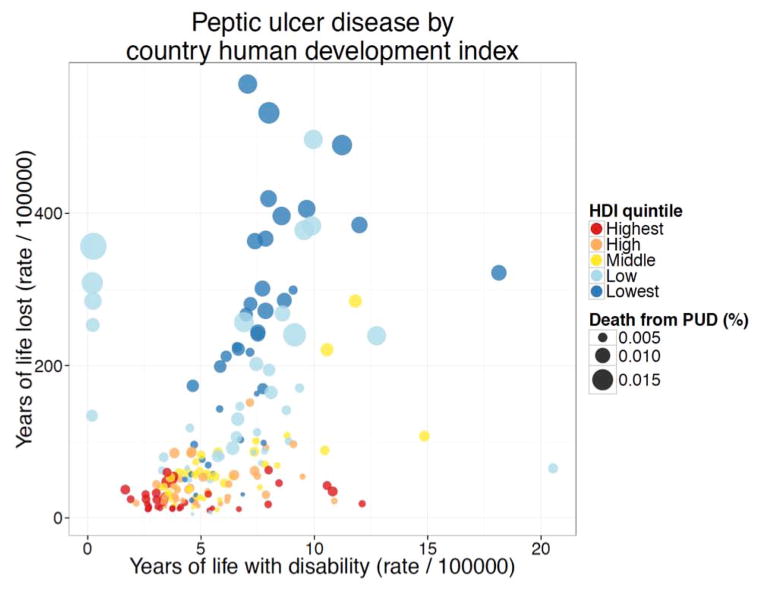
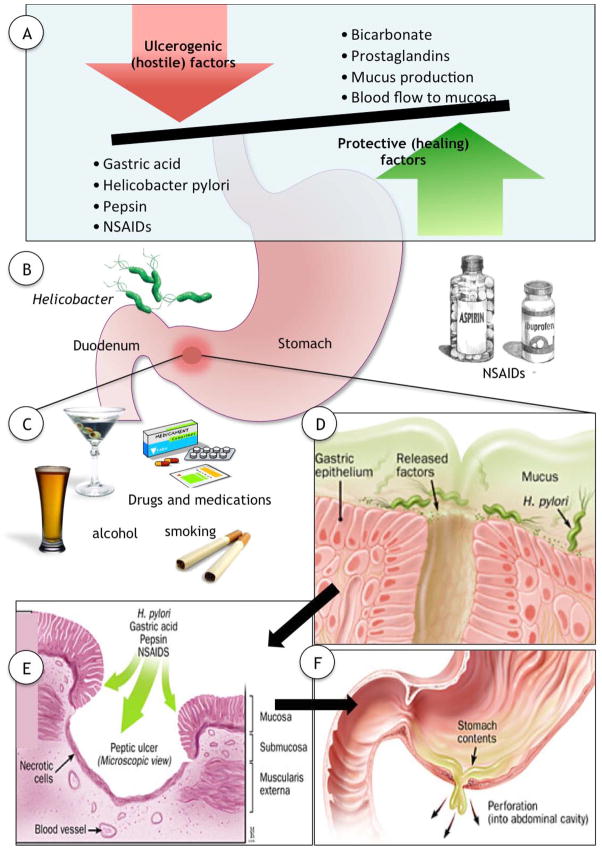
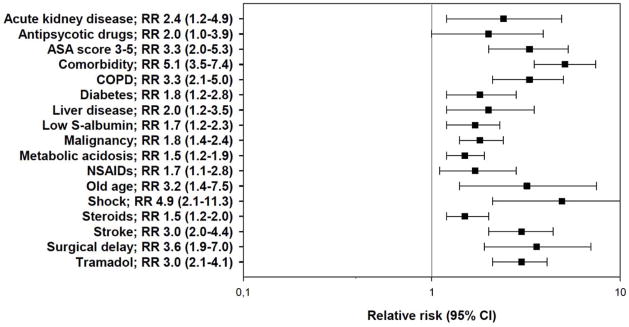
Perforated peptic ulcer is a common emergency condition worldwide, with associated mortality rates of up to 30%. A scarcity of high-quality studies about the condition limits the knowledge base for clinical decision making, but a few published randomised trials are available. Although Helicobacter pylori and use of non-steroidal anti-inflammatory drugs are common causes, demographic differences in age, sex, perforation location, and underlying causes exist between countries, and mortality rates also vary. Clinical prediction rules are used, but accuracy varies with study population. Early surgery, either by laparoscopic or open repair, and proper sepsis management are essential for good outcome. Selected patients can be managed non-operatively or with novel endoscopic approaches, but validation of such methods in trials is needed. Quality of care, sepsis care bundles, and postoperative monitoring need further assessment. Adequate trials with low risk of bias are urgently needed to provide better evidence. We summarise the evidence for perforated peptic ulcer management and identify directions for future clinical research.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
KS – None
KT – None
EMH - None
JB - None
MHM - None
MYO - None
JAS - None
Figures
References
-
- Møller MH, Adamsen S, Thomsen RW, et al. Multicentre trial of a perioperative protocol to reduce mortality in patients with peptic ulcer perforation. Br J Surg. 2011;98(6):802–10. - PubMed
-
- Malfertheiner P, Chan FK, McColl KE. Peptic ulcer disease. Lancet. 2009;374(9699):1449–61. - PubMed
-
- Lau JY, Barkun A, Fan DM, et al. Challenges in the management of acute peptic ulcer bleeding. Lancet. 2013;381(9882):2033–43. - PubMed
-
- Wang YR, Richter JE, Dempsey DT. Trends and outcomes of hospitalizations for peptic ulcer disease in the United States, 1993 to 2006. Ann Surg. 2010;251(1):51–8. - PubMed
-
- Lau JY, Sung J, Hill C, et al. Systematic review of the epidemiology of complicated peptic ulcer disease: incidence, recurrence, risk factors and mortality. Digestion. 2011;84(2):102–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
