

Prevalence of Prostate Cancer Clinical States and Mortality in the United States: Estimates Using a Dynamic Progression Model
- PMID: 26460686
- PMCID: PMC4603789
- DOI: 10.1371/journal.pone.0139440
Prevalence of Prostate Cancer Clinical States and Mortality in the United States: Estimates Using a Dynamic Progression Model
Abstract
Objective: To identify patient populations most in need of treatment across the prostate cancer disease continuum, we developed a novel dynamic transition model based on risk of disease progression and mortality.
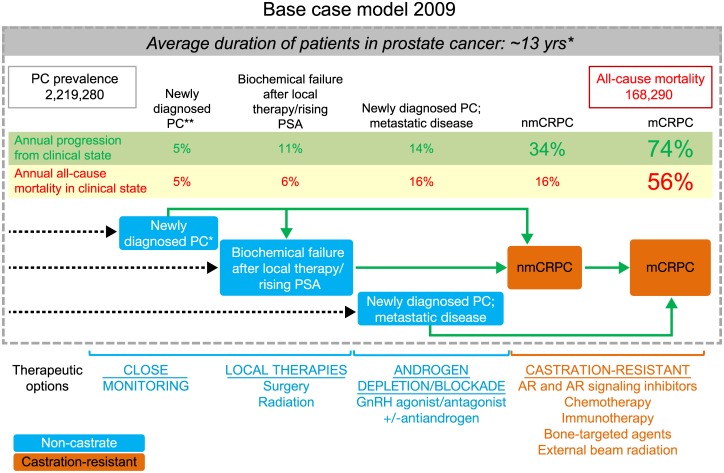
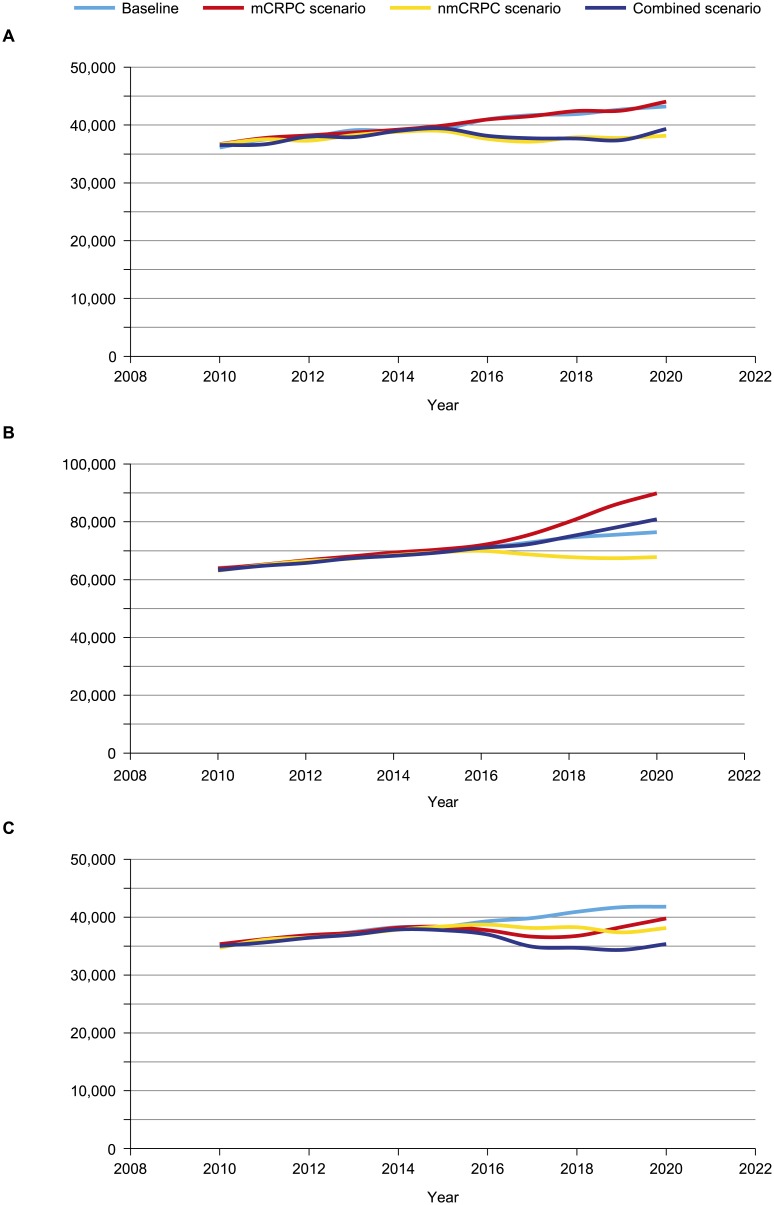
Design and outcome measurements: We modeled the flow of patient populations through eight prostate cancer clinical states (PCCS) that are characterized by the status of the primary tumor, presence of metastases, prior and current treatment, and testosterone levels. Simulations used published US incidence rates for each year from 1990. Progression and mortality rates were derived from published clinical trials, meta-analyses, and observational studies. Model outputs included the incidence, prevalence, and mortality for each PCCS. The impact of novel treatments was modeled in three distinct scenarios: metastatic castration-resistant prostate cancer (mCRPC), non-metastatic CRPC (nmCRPC), or both.
Results and limitations: The model estimated the prevalence of prostate cancer as 2,219,280 in the US in 2009 and 3,072,480 in 2020, and incidence of mCRPC as 36,100 and 42,970, respectively. All-cause mortality in prostate cancer was estimated at 168,290 in 2009 and 219,360 in 2020, with 20.5% and 19.5% of these deaths, respectively, occurring in men with mCRPC. The majority (86%) of incidence flow into mCRPC states was from the nmCRPC clinical state. In the scenario with novel interventions for nmCRPC states, the progression to mCRPC is reduced, thus decreasing mCRPC incidence by 12% in 2020, with a sustained decline in mCRPC mortality. A limitation of the model is that it does not estimate prostate cancer-specific mortality.
Conclusion: The model informs clinical trial design for prostate cancer by quantifying outcomes in PCCS, and demonstrates the impact of an effective therapy applied in an earlier clinical state of nmCRPC on the incidence of mCRPC morbidity and subsequent mortality.
Conflict of interest statement
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2014. Atlanta: American Cancer Society; 2014.
-
- Mohler JL, Armstrong AJ, Bahnson RR, Boston B, Busby JE, D'Amico AV, et al. NCCN clinical guidelines in oncology—prostate cancer. Version I.2015. National Comprehensive Cancer Network Web site. Available: http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.
-
- Scher HI, Heller G. Clinical states in prostate cancer: toward a dynamic model of disease progression. Urology. 2000;55(3): 323–7. - PubMed
-
- Solo K, Mehra M, Dhawan R, Valant J, Scher HI. Prevalence of prostate cancer (PC) clinical states (CS) in the United States: estimates using a dynamic progression model. J Clin Oncol. 2011;29(Suppl). Abstract 4637.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
