

Primary CNS lymphoproliferative disease, mycophenolate and calcineurin inhibitor usage
- PMID: 26460822
- PMCID: PMC4741807
- DOI: 10.18632/oncotarget.5292
Primary CNS lymphoproliferative disease, mycophenolate and calcineurin inhibitor usage
Abstract
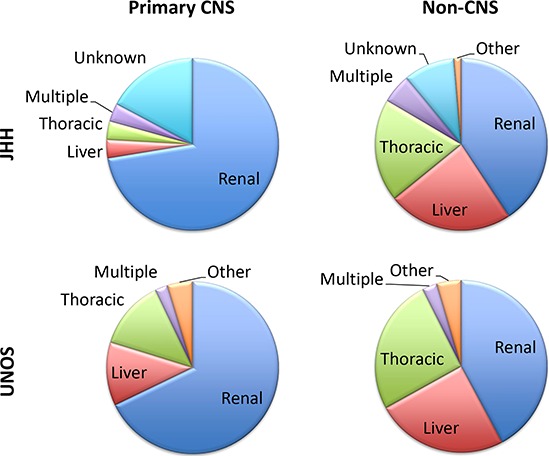
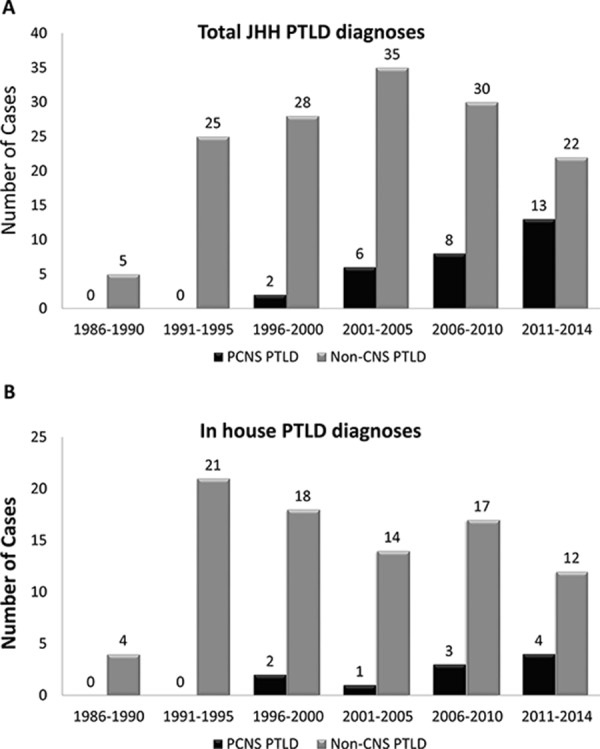
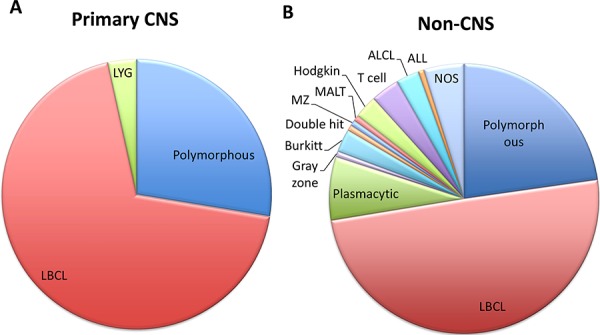
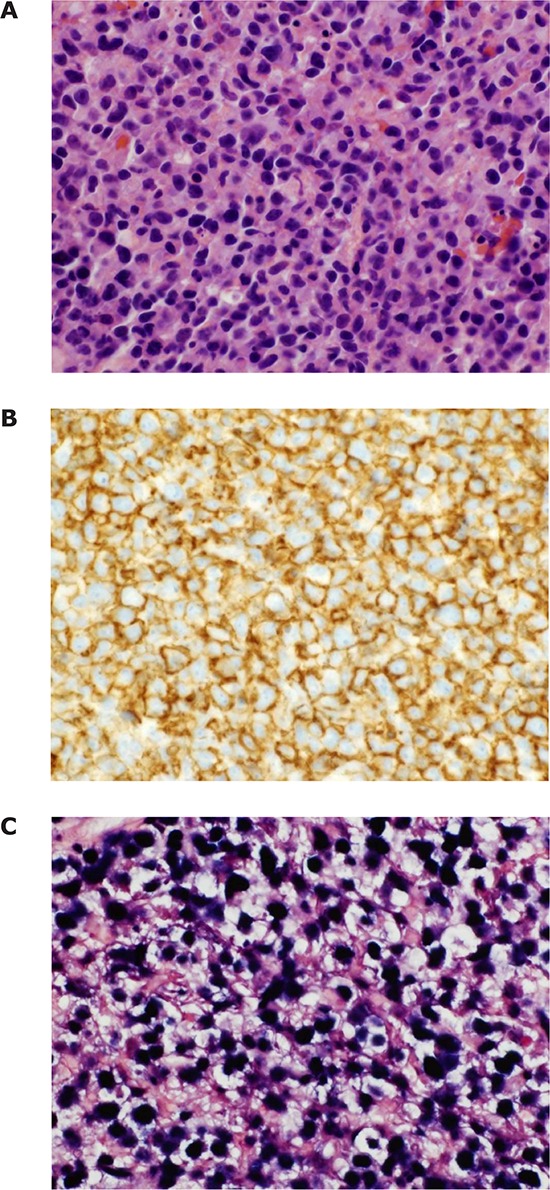
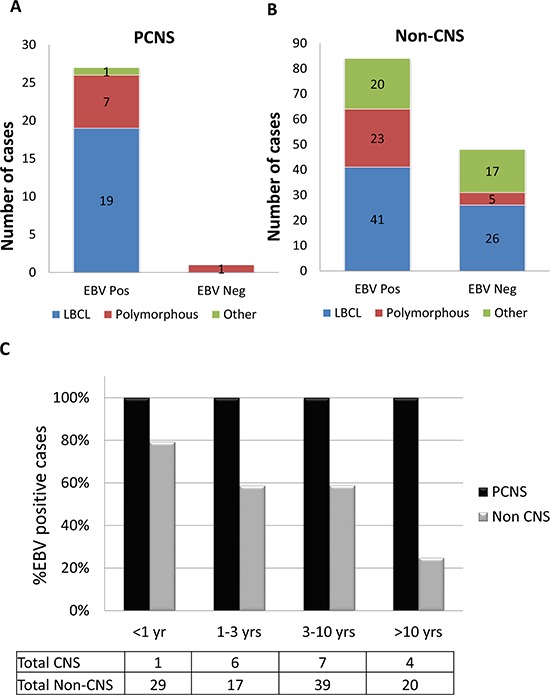
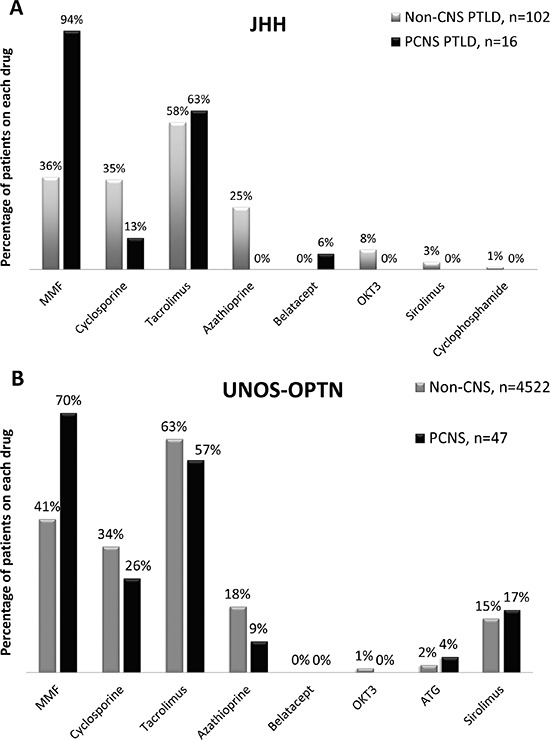
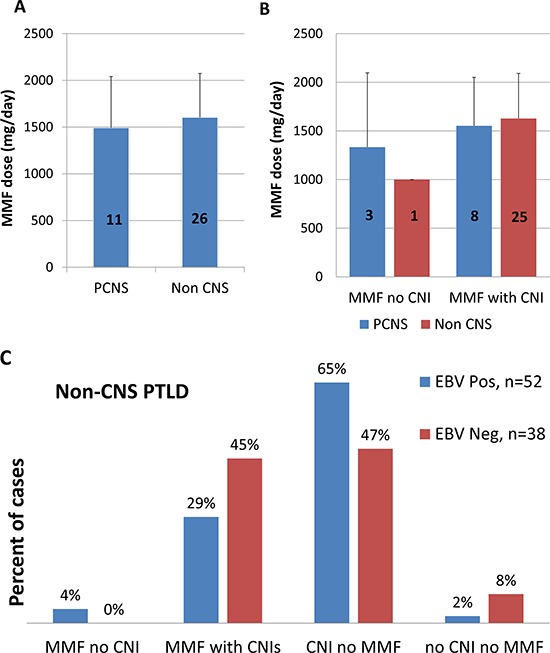
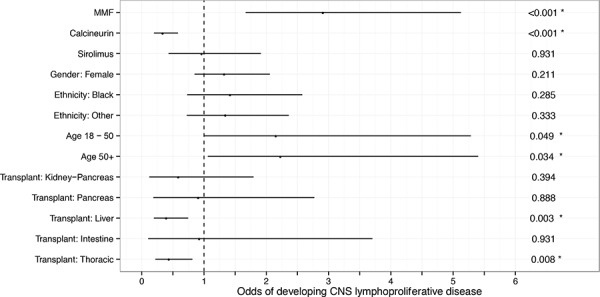
Immunosuppression for solid organ transplantation increases lymphoproliferative disease risk. While central nervous system (CNS) involvement is more rare, we noticed an increase in primary CNS (PCNS) disease. To investigate a potential association with the immunosuppressive regimen we identified all post-transplant lymphoproliferative disease (PTLD) cases diagnosed over a 28-year period at our institution (174 total, 29 PCNS) and all similar cases recorded in a United Network for Organ Sharing-Organ Procurement and Transplant Network (UNOS-OPTN) datafile. While no PCNS cases were diagnosed at our institution between 1986 and 1997, they comprised 37% of PTLD cases diagnosed from 2011-2014. PCNS disease was more often associated with renal vs. other organ transplant, Epstein-Barr virus, large B-cell morphology and mycophenolate mofetil (MMF) as compared to PTLD that did not involve the CNS. Calcineurin inhibitors were protective against PCNS disease when given alone or in combination with MMF. A multivariate analysis of a larger UNOS-OPTN dataset confirmed these findings, where both MMF and lack of calcineurin inhibitor usage were independently associated with risk for development of PCNS PTLD. These findings have significant implications for the transplant community, particularly given the introduction of new regimens lacking calcineurin inhibitors. Further investigation into these associations is warranted.
Keywords: Epstein-Barr virus; calcineurin inhibitors; mycophenolate mofetil; post-transplant lymphoproliferative disorder; primary central nervous system lymphoma.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Opelz G, Döhler B. Lymphomas after solid organ transplantation: a collaborative transplant study report. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2004;4:222–230. - PubMed
-
- Opelz G, Henderson R. Incidence of non-Hodgkin lymphoma in kidney and heart transplant recipients. Lancet. 1993;342:1514–1516. - PubMed
-
- Cherikh WS, Kauffman HM, McBride MA, Maghirang J, Swinnen LJ, Hanto DW. Association of the type of induction immunosuppression with posttransplant lymphoproliferative disorder, graft survival, and patient survival after primary kidney transplantation. Transplantation. 2003;76:1289–1293. - PubMed
-
- Swinnen LJ, Costanzo-Nordin MR, Fisher SG, O'Sullivan EJ, Johnson MR, Heroux AL, Dizikes GJ, Pifarre R, Fisher RI. Increased incidence of lymphoproliferative disorder after immunosuppression with the monoclonal antibody OKT3 in cardiac-transplant recipients. The New England journal of medicine. 1990;323:1723–1728. - PubMed
-
- Caillard S, Dharnidharka V, Agodoa L, Bohen E, Abbott K. Posttransplant lymphoproliferative disorders after renal transplantation in the United States in era of modern immunosuppression. Transplantation. 2005;80:1233–1243. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
